Ladies and gentlemen,
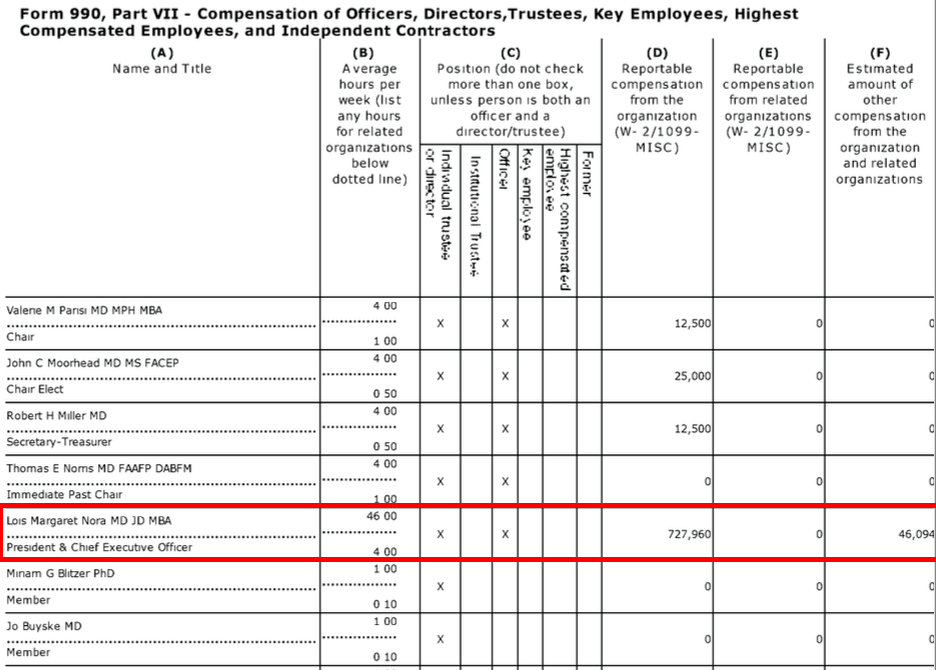
With the cooler temperatures, kids heading back to school, and a new fall season soon upon us, there's excitement building in the air! The much-coveted position at the American Board of Medial Specialties (ABMS), President and CEO, will soon be vacant. In October, 2016, Lois Nora, MD, JD, MBA announced her upcoming retirement in December of this year after six years of leadership and the political jostling for her comfy salary, first class travel, and health/social club membership perks have been underway for some time.
Who will be her lucky successor? For that matter, who might be potential candidates for her position?
This is an important consideration for US physicians who increasingly find their ability to practice medicine compromised by the proprietary ABMS Maintenance of Certification® (MOC®) program. Since working physicians in America have no control over the selection of this lucky person, we can only venture a guess who might be considered. But there have been several recent hints in various media channels who might be throwing their hat in the ABMS-leadership ring.
Here is a recent sampling:
1) Hal C. Lawrence III, MD - Executive Vice President and CEO of the American College of Obstetrics and Gynecology (ACOG)
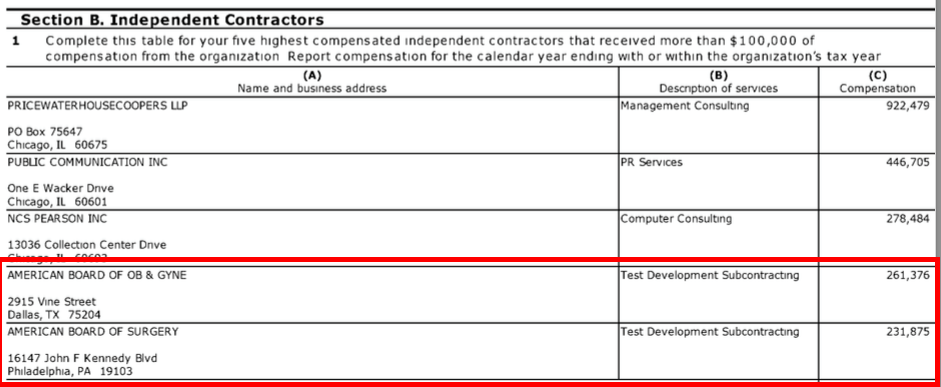
Dr. Lawrence has demonstrated leadership and political moxie drafting the recent letter reportedly "signed" by 38 state medical societies and 33 medical specialty societies in support of a "re-directed" form of MOC® that helps preserves our current highly conflicted method of "professional self-regulation." Dr. Lawrence has also proven himself capable at helping preserve the American Board of Obstetrics and Gynecology subcontractor role as test developers for the ABMS if the status quo is continued. For these reasons, Dr. Lawrence appears well on his way as a possible Dr. Nora replacement.
2) Yul Enjes, MD or 3) Eric Green, MD - a.k.a. "The Doctors Who Defend MOC"
Dr. Enjes has first-hand experience with political cronyism in non-profits serving on the ABIM Board of Directors and as former Chair of the American College of Physicians Board of Governors. Dr. Enjes has cleverly laid low on his important role with supporting MOC - until this article - and can't believe state legislators should have a role protecting the doctor-patient relationship when the ABIM's practices of strong-arming physicians to spend $23,607 every ten years for their condo puchases has been so effective. As such, Dr. Enjes seems like a real ABMS team player!
Dr. Green, on the other hand, might be an equally formidable candidate since he appears to be a strong proponent of income distribution in the form of a "minor" MOC "tax on our time to help the public." His convenient ability of forgetting to mention there is no independent proof that MOC® helps anyone except ABMS revenues makes him a strong candidate for Dr. Nora's position, or any other ABMS member board.
4) Richard Baron, MD - war-torn but time-tested President and CEO of the American Board of Internal Medicine (ABIM) and ABIM Foundation.
There isn't a handsome salary out there Dr. Baron would refuse without having to see patients and Dr. Baron's former work at the Seamless Care Models Group at the Center for Medicare and Medicaid Services to secure MOC® as an (unproven) quality metric gives him a leg up on the other candidates. The only problem now is that Dr. Baron would have to accept a pay cut relative to his robust $849,483/year haul he receives from the ABIM and ABIM Foundation. Still, the ability to spend more time away from the office without the frontline controversy created by the ABIM Foundation's $2.3 million condominium purchase, ongoing anti-trust and physician suits, Cayman Island fund transfers and controversial income redistribution plans using ABIM diplomate testing fees to provide "grants" for various forms of "professionalism" in our nation's medical schools might be welcomed as the heat continues to be applied at the ABIM.
5) Darryl S. Weiman, MD, Professor of Surgery, University of Tennessee Health Science Center and author of "Maintaining My Surgical Certification" in The Huffington Post.
Dr. Weiman, who conveniently fails to mention the American Board of Surgery's conflicts in test development for the ABMS in his HuffPo piece, might be a shoe-in for the position since he appears to be facile at spouting veiled threats in the politically liberal US news and opinion media outlets like the Huffington Post. No doubt the ABMS board of directors love hearing him threaten that loss of maintenance of certification would mean "the public may perceive this as a nefarious way for the medical profession to lower its standards." Wow. Powerful stuff that means nothing to real patients. Since Dr. Weiman seems blind to the nefarious ways the ABMS MOC® program discriminates against younger physicians, uses undisclosed strongmen for protection, and promotes the use of our testing fees for their personal use, it's hard to see how such a fine candidate for Dr. Nora's position could possibly be passed over.
It's a crowded field already.
So who will be Dr. Nora's replacement? Will it be one of these folks or someone else? (The ABMS really needs your help deciding. Comments open.)
-Wes
Thursday, August 31, 2017
{kind=link}
{kind=link}
{kind=link}
Friday, August 25, 2017
On State Medical Societies' Letter to End or "Redirect" MOC
I was intrigued that a number of professional subspecialty societies joined with the state medical societies to request a meeting on 4 Dec 2017 with Dr. Nora to voice their concerns about MOC with the ABMS. Whether the ABMS will agree to a meeting or just use this meeting as another example of "listening" to more groups before fulfilling their own agenda remains to be seen. What is concerning to me, however, is that state medical societies felt they needed to ask Dr. Nora for a meeting when they are the ones that hold the ultimate accountability of self-regulation in their respective states. Shouldn't Dr. Nora be asking for a meeting with them? And why request a meeting with Dr. Nora on 4 December 2017 when she's planning on retiring later the same month?
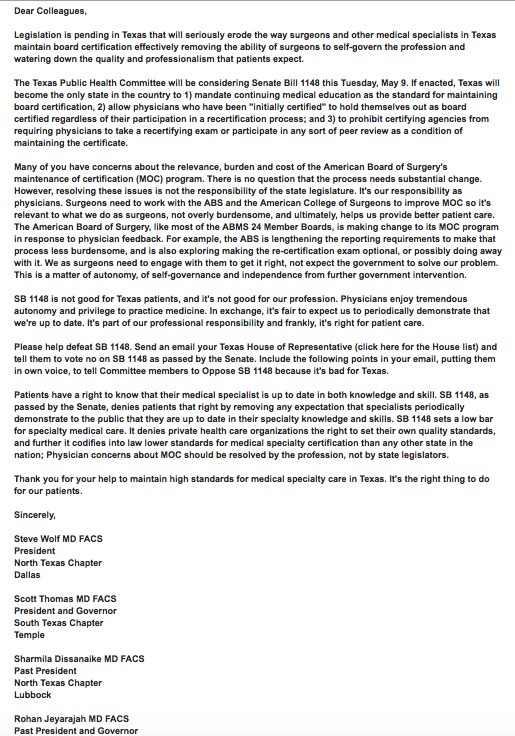
I worry about the political and business naïveté' of these state medical organizations relative to the specialty societies who earn considerable annual revenues from MOC and may be recruiting them. It is concerning that the circulated letter uses the same talking points as the ABMS and their member boards. This letter quickly shifts from the concerns about MOC to the talking point that "this is not about MOC but professional self-regulation." The same concern of the potential loss of "professional self-regulation" recently appeared in a JAMA opinion piece supportive of MOC by a former American Board of Internal Medicine board director. It was also mentioned in an earlier May, 2017 email blast from the American College of Surgeons who opposed the anti-MOC legislation in Texas. Impressive "harmonization?"
{kind=link}
There appears to be a consensus that using the strategy of holding loss of professional self-regulation over working physicians' heads will help us forget all that pesky corruption. Surely state medical societies do not want to buy into this kind of manipulation. Pity the poor physician who does not want to lose his ability to self-regulate his profession and rejects corruption. Where are they to stand? Might this talking point "harmonization" actually be a means to legitimize a "redirected" version of MOC?
The only thing I might say in reply is these organizations only took us half way there.
The current tone of this letter is not one of intolerance and repudiation of the corrupt ABMS MOC program, but rather a request to "redirect" it. In fact, this letter has a disconnect between wanting to "redirect" MOC with only two choices for practicing physicians: (1) propping up the current system of "professional self-regulation" or (2) something else. There is no clarity to the "something else." This is analogous to telling physicians that we'd better slip the Chicago alderman $200 per year, and be grateful for the protection. Why would state medical societies join in such a veiled threat?
Our current method of ABMS member board "professional self-regulation" using MOC has proven itself to be corrupt and laden with numerous undisclosed conflicts of interest, self-dealing, non-transparency, and intimidating strongman tactics. Should we be grateful to ABMS for this, given the nebulous alternative? Let's get the ominous alternative on the table. And why in this letter is there no possibility of a third choice when an alternative model to MOC is developing in front of our eyes?
Naturally, the National Board of Physicians and Surgeons (NBPAS) has a monumental shortcoming. It fails to guarantee millions in educational fees to many of the subspecialty societies on this letter. One can see how this third possibility just isn't as, well, fun.
Perhaps that's the real reason this letter was released.
Physician members of these specialty and state medical societies should be aware they are playing into ABMS's hand with this letter and should be up to date on the options and the evolving consensus regarding legitimate professional self-regulation. To that end, the integrity and transparency of the NBPAS should be promoted in lieu of the ABMS. Indeed, the state medical societies of Texas and Pennsylvania have played important roles in placing physicians and their patients before the financial concerns of subspecialty organizations and ABMS member boards. This should set a precedent for state medical societies across the country. What they should NOT be doing is begging for a meeting with a lame duck President and CEO of the ABMS who are only looking to grow the frequency and cost of MOC in the name of "professional self-regulation" since the ABMS and their member boards are the ones that got us in this mess in the first place.
Radical reform of the corrupt MOC program is not paying the Chicago alderman $250 per year instead of $200.
- Wes
Addendum 26 Aug 2017 06:23AM - Appendix B added and the origin of the letter (AAMSE) added.
* That individual, Hal C. Lawrence III, MD, ACOG Executive Vice President and CEO, has significant conflicts of interest with the ABMS. The American College of Obstetrics and Gynnecology (ABOG) are subcontractors for "Test Development" with the ABMS.
Wednesday, August 16, 2017
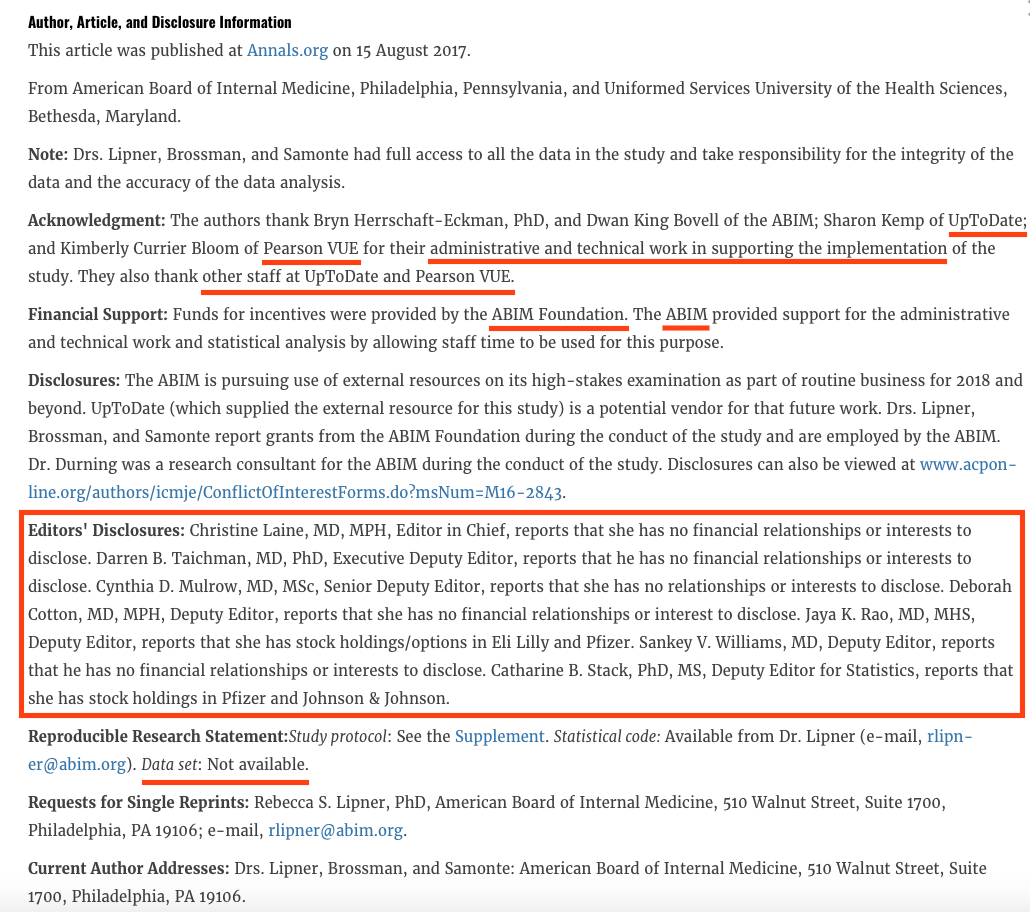
Fake News: Annals of Internal Medicine's Disclosures
The article touted a comparison between open book vs. closed book testing that was conceived exclusively by the American Board of Internal Medicine and executed by their conflicted corporate partners at PearsonVue and a new $10.5 billion corporate heavyweight from the Netherlands, Wolters Kluwer. In a veiled attempt at full disclosure, the conflicts of interest of the study were carefully articulated in a lengthy disclosure statement hidden behind a paywall. True to form, nearly all of the editors of the article claimed "no financial relationships or interests to disclose."
{kind=link}
Most internists in the U.S. know these editors' disclosure is little more than fake news. The Annals of Internal Medicine is an academic medical journal published by the American College of Physicians (ACP). On its last available Form 990, the ACP earned over $24.6 million in a single year selling their Medical Knowledge Self-Assessment Program to US physicians to study for their board certification and recertification examinations. Even the accompanying editorial was written by ACP's former senior executive vice president, Steven E. Weinberger, MD, who disclosed he was an employee of the ACP and earned royalties from authored material on UpToDate.
.png){kind=link}
In addition, the supplement supplied by the authors had portions of the recruiting notice redacted so avoid true disclosure. But when a copy of the actual recruiting notice is revealed here, it is clear that PearsonVue had more than a minor role in the research and had access to the study registrants' names, addresses, and probably more.
.jpg){kind=link}
Each of the 825 physicians enrolled in the study received $250, costing US physicians (who unwittingly funded the ABIM Foundation) $206,250 for "incentive payments" for this study, not including the time and salaries of those who conducted this study for the ABIM's benefit. None of the participants were told about the financial benefits to the ABIM, PearsonVue, Wolters Kluwer, or their content creators for participation in this study.
Such conflicted "research" published in an academic medical journal that misleads the public and US physicians represents little more than a free advertisement for the financial agendas of these colluding organizations and sets and incredibly low (and untrustworthy) bar for all of academic publishing.
-Wes
Tuesday, August 15, 2017
Texas to JAMA: A Lesson on Self-Regulation
Texas Medical Association (TMA) spent no time responding to David H. Johnson, MD's veiled threat of loss of self-regulation with the passage of Texas Anti-MOC legislation, SB1148, published in JAMA 7 Aug 2017:
-Wes
In a letter to the editor submitted to JAMA but not yet published, TMA President Carlos J. Cardenas, MD, agrees on the importance of self-regulation to his profession.Here's a link to the full statement.
"It encompasses our responsibility and our authority to establish and enforce standards of education, training, and practice," Dr. Cardenas wrote. "We routinely defend that responsibility and authority in advocating against the intrusion of all third parties — such as government, private insurers, hospital administrators — into the practice of medicine."
But physicians in Texas and across the country, he argued, do not see the certifying boards as "self."
"They are, instead, profit-driven organizations beholden to their own financial interests," Dr. Cardenas wrote. "In fact, they are now one of the outsiders intruding into the practice of medicine."
Until the boards "completely overhaul their processes, finances, and lack of transparency," he concluded, physicians "will have no choice but to continue to seek statutory defenses against these third-party intrusions into our noble profession."
-Wes
Friday, August 11, 2017
MOC and Recertification - As Predicted
David H. Johnson, MD, former board member of the American Board of Internal Medicine (ABIM), authored an opinion piece entitled "Maintenance of Certification and Texas Bill SB1148 - A Threat to Professional Self-Regulation" in the August 7th issue of JAMA. At the end of his article, Dr. Johnson discloses that he served as a member of the American Board of Internal Medicine board of directors from 2007 until 2015 and as board chair from 2013 until 2015.
Dr. Johnson's leadership and influence at the ABIM spanned the time of the purchase of the ABIM Foundation $2.3 million condominium in December 2007, the hiring of the ABIM's felonious "Director of Investigations" (formerly "Director of Test Security") in 2008, the Arora Board Review sting operation in 2009, blind approval of Christine Cassel, MD's conflicts as she simultaneously served on the boards of Kaiser Foundation and Hospitals and Premier, Inc., approval of a $1.2 million golden parachute for Dr. Cassell as she left for the National Quality Forum, and the appointment of Richard Baron, MD who served revolving-door positions from the ABIM, the Center for Medicare and Medicaid Services, the National Quality Forum, and back to the ABIM as he worked to create "seamless" care models for their organization and others.
Dr. Johnson tries to defend MOC by referring to an opinion piece published in 1979 by Arnold S. Relman, MD (who as the editor of the New England Journal of Medicine at the time and a staunch single-payer advocate). But Dr. Johnson failed to mention Dr. Relman's prescient predictions for recertification shortly after introduction of the exercise over 40 years ago:
... just as Dr. Relman predicted.
-Wes
Dr. Johnson's leadership and influence at the ABIM spanned the time of the purchase of the ABIM Foundation $2.3 million condominium in December 2007, the hiring of the ABIM's felonious "Director of Investigations" (formerly "Director of Test Security") in 2008, the Arora Board Review sting operation in 2009, blind approval of Christine Cassel, MD's conflicts as she simultaneously served on the boards of Kaiser Foundation and Hospitals and Premier, Inc., approval of a $1.2 million golden parachute for Dr. Cassell as she left for the National Quality Forum, and the appointment of Richard Baron, MD who served revolving-door positions from the ABIM, the Center for Medicare and Medicaid Services, the National Quality Forum, and back to the ABIM as he worked to create "seamless" care models for their organization and others.
Dr. Johnson tries to defend MOC by referring to an opinion piece published in 1979 by Arnold S. Relman, MD (who as the editor of the New England Journal of Medicine at the time and a staunch single-payer advocate). But Dr. Johnson failed to mention Dr. Relman's prescient predictions for recertification shortly after introduction of the exercise over 40 years ago:
"Now there are signs that the boards and many of the specialty societies are beginning to have second thoughts about the whole idea of recertification. At the meeting last March of the American Board of Medical Specialties, delegates had such misgivings that they could not agree on whether a specialist's recertification status should even be mentioned in the Directory of Medical Specialists. The Council of Medial Specialty Societies reports that at least four of its constituents societies (representing dermatology, neurological surgery, orthopedic surgery, and radiology) now oppose the idea of recertification, and other societies are said to have 'sizable blocs of members with serious reservations.' At the recent meeting of the AMA's House of Delegates in Chicago, a resolution was taken under consideration that recommends that all specialty boards except Family Practice call a moratorium of recertification. The intent of the resolution is to put an emphasis on mandatory continuing medical education (CME) as a preferred alternative to any kind of recertification program. It is still too early to know whether these developments portend a decisive change in organized medicine's attitude toward recertification, but what seems clear is that the recertification process no longer commands widespread confidence, if it ever did. ... Many doctors are worried that many perfectly competent and conscientious practitioners might be unable to pass recertifying examinations that emphasize arcane facts and the latest literature rather than the practical management of patients. Many doctors also suspect that even voluntary programs would inevitably become compulsory and that the whole recertification process would soon come under government scrutiny and ultimately government control. Reimbursement schedules and hospital staff appointments might then be determined by recertification status; in consequence specialists unable to meet arbitrarily imposed examination standards might find their livelihood in jeopardy."Dr. Relman's prescient predictions are now most practicing physicians' reality. There is a certain schadenfreude that exists with the physician community toward the ABIM since passage of Texas anti-MOC legislation, SB1148. The ABMS Member boards (and the ABIM in particular) are responsible for Texas Bill SB1148, not practicing physicians. The threat to practicing physicians is not the loss of self-regulation, as Dr. Johnson surmises. Rather, it is loss of trust in the US physician credentialing system that has been spawned by the threats, intimidation and indifference to fraud by members of our bureaucratic physician academic elite within the credentialing community because of the huge profits and control over physicians it generates for their own purposes...
... just as Dr. Relman predicted.
-Wes
Sunday, August 06, 2017
ABMS Reacts to JAMA MOC Financial Study

Let's fact-check their public statement line by line:
"The research letter entitled 'Fees for Certification and Finances of Medical Specialty Boards' published in the Aug. 1, 2017 issue of JAMA offers an aggregate view of the fees charged by the 24 ABMS Member Boards for more than 860,000 physicians to obtain initial Board Certification and as well as continuing certification throughout a physician's career.Note the ABMS rebuttal statement was careful not to use the term Maintenance of Certification® (MOC®), but rather used the term "continuing certification." That's because it would hint at the existence of their for-profit wholly-owned subsidiary, ABMS Solutions, LLC, domiciled in Atlanta, GA, that makes money selling physician MOC® certification status to third parties, generating revenues in excess of those disclosed in their rebuttal statement or in the original JAMA research letter.
"According to the letter, the 2013 Member Boards' revenue represents approximately $313 per ABMS Board Certified physician. This is a reasonable amount to support a nationally recognized credentialing program that is both respected and valued by physicians, healthcare providers, and institutions, and most importantly, patients and their families.In fact, 81% of physicians feel MOC® is a burden and only 15% felt recertification was worth the effort. Independent studies have failed to identify a difference in time-limited versus lifetime-certified physicians, reinforcing the fact that MOC® is little more than a revenue generator for the ABMS. Also, the ABMS is careful not to mention the word "annually" in their statement when they describe the revenue generated per ABMS Board Certified physician. It is also strange that the ABMS would call their fees "reasonable" when those fees only apply to new, younger, often debt-burdened physicians and not to older physicians certified before 1990. Older physicians are not required to participate in MOC® to keep hospital privileges or insurance panel payments. Age discrimination - a hallmark of the ABMS MOC® program - is not "reasonable" to any ethical working physician or member of the public.
"In addition, the estimated annual cost for continuing certification of $257 per ABMS Board Certified physician is an acceptable cost for physicians to demonstrate that they have the current knowledge, judgment, and skills to provide the highest level and most up-to-date care to their patients.Funny how this number that pays salaries that are over four times the average physician's salary are deemed "reasonable" for member boards of the ABMS. $257 stands in stark contrast to the competing certifying board, the National Board of Physicians and Surgeons (nbpas.org) whose fees are only $84.50 per year and is equally credible - if not more so - since their Boards' leadership are unpaid.
"IRS Form 990 provides information regarding revenues, expenditures, and assets. However, they do not outline the actual operation cost involved in creating, sustaining, and implementing a rigorous and comprehensive process of Board Certification and continuing certification for the nation's physicians. ABMS Member Boards rely on a highly trained and specialized work force including psychometricians, assessment professionals, and medical educators to develop, evaluate, and administer Board Certification programs.Those fees also paid for a felonious strongman to overstep their authority to intimidate vulnerable physicians by secretly audiotaping a competing ACGME-accredited board review course. Using those audiotapes the ABIM obtained permission to raid the course director's home to seize his computers so the ABIM staff could track physician attendees' email addresses and accusing them of violating ABIM's "pledge of honesty." These activities are more akin to a protection racket rather than a physician continuing education/credentialing system.
The ABMS member boards also have numerous large, undisclosed financial conflicts of interest. For instance, in fiscal year 2013, the ABIM paid their non-physician Chief Operating Officer, Ms. Lynn Langdon, over $464,747 while Christine Cassel, MD (President and CEO of the ABIM and its Foundation) earned $838,603 from physicians while she simultaneously served on the Boards of Kaiser Foundation and Hospitals and Premier, Incorporated, the largest hospital purchasing agent that also does "performance improvement consulting" for over 2,900 US hospitals. True to form: the ABMS never mentions these additional conflicts of interest in their statement.
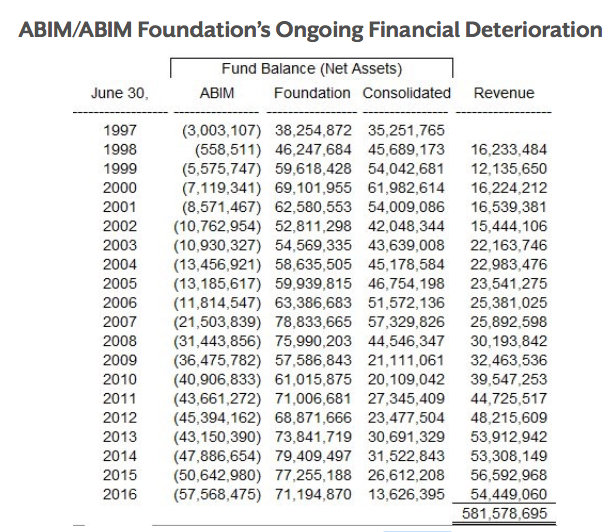
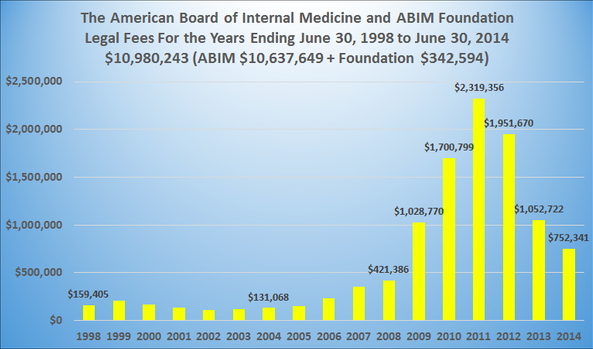
"For this reason, the greatest expenditure is appropriately in the area of staff salary and compensation, as noted in their 990 reports. "The assets reported on the IRS Form 990 that the ABMS Member Boards currently maintain are crucial to sustain and evolve vibrant and innovative Board Certification and continuing certification programs. ABMS Member Boards are continually reinvesting in program improvements and enhancements to transform their certification and continuing certification programming, including the development of quality improvement and longitudinal assessment programs.Those "vibrant and innovative enhancements" include a $2.3 million condominium complete with a chauffeur-driven town car, investments in the Cayman Islands, for-profit real estate ventures, and even a pond. The largest member board, which secretly channeled over $77 million of physician testing fees to create their ABIM Foundation from 1990 through 2007, now only has $13.6 million remaining in their latest consolidated financials thanks to high salaries and mounting legal fees. I'm not sure I can remember a time of so much innovation (and cover-up) in physician certification!
{kind=link}
{kind=link}
"These investments will ensure that ABMS Board Certification continues to be a relevant, valued, and important quality indicator for those who hold the credential as well as those who rely upon it for the highest standard of quality care."Unfortunately, the ABMS member boards have enjoyed a sheltered workshop for years that the internet has thoroughly disrupted. Sadly, physicians no longer trust the ABMS and their member boards to act in their interest or in the interest of the public. Instead, the data are overwhelming now that the ABMS and their member boards are more concerned about themselves than the public. As such, their tax exempt status should be challenged.
The question now is, are there any investigators/prosecutors at the IRS that will investigate this potential fraud, or are they beholden to the highly political Medical Industrial Complex, too?
-Wes
Image credit: Medscape.
Thursday, August 03, 2017
Direct Adverse Effects of MOC® on Patients
The American Board of Medical Specialties (ABMS) successfully lobbied to have their proprietary Maintenance of Certification® (MOC®) program included in the new Merit-Based Incentive Payment Program of the new Center for Medicare and Medicaid Services (CMS) "quality payment program" within Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) legislation. Hospitals and insurers continue to demand MOC® recertification of their physicians without asking a most important question: has MOC® been harmful to patients or their physicians?
Here are real life examples of how the ABMS MOC® program has been harmful to patients:
Example #1, Dr. J.E. of New Jersey
From antitrust legislation before the Northern District of Illinois Federal District Court, Case 1:14-cv-02705:
- Wes
Here are real life examples of how the ABMS MOC® program has been harmful to patients:
Example #1, Dr. J.E. of New Jersey
From antitrust legislation before the Northern District of Illinois Federal District Court, Case 1:14-cv-02705:
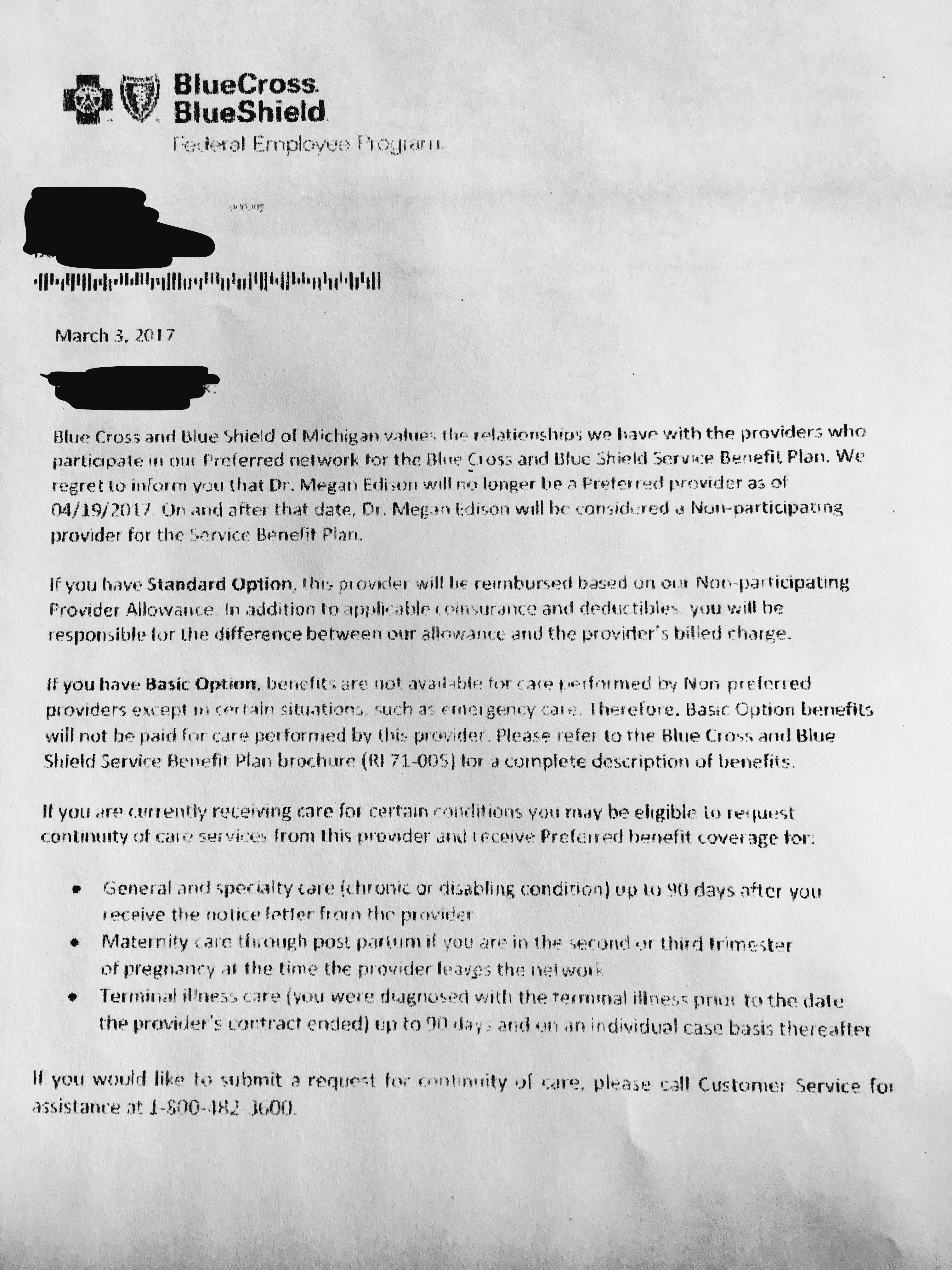
Association of American Physicians & Surgeons, Inc. v. American Board of Medical SpecialtiesExample #2 Megan Edison, MD of Michigan
Assigned to: Honorable Andrea R. Wood
Case in other court: New Jersey, 3:13-cv-02609
Cause: 15:1 Antitrust Litigation
"
Exclusion of an AAPS Member from Somerset Medical Center (SMC)
29. Defendant ABMS’s foregoing agreements and actions resulted in the unjustified exclusion of a physician member of Plaintiff AAPS (“J.E.”) from the medical staff at SMC, a hospital located in Somerville, New Jersey.
30. Physician J.E. had been on the SMC medical staff to treat patients there for twenty-nine (29) years.
31. J.E. had been board certified by The American Board of Family Practice, which subsequently changed its name to The American Board of Family Medicine (“ABFM”).
32. In 2011, SMC refused to allow J.E. to remain on its medical staff unless he complied with an extremely burdensome and impractical recertification procedure under the ABMS MOC®.
33. ABFM is one of the 24 corporations identified above that has agreed with Defendant ABMS to implement ABMS MOC®.
34. Although J.E. had been fully certified in good standing with the predecessor to ABFM, Defendant’s agreement with ABFM required imposing the following extremely burdensome requirements for recertification under ABMS MOC®:
35. The foregoing requirements demand far in excess of 100 hours for a typical physician, with the possibility of an unjustified rejection of recertification for reasons having no proven connection with patient care.
- Completion of fifty (50) MC-FP points (acquired by doing modules)
- Minimum of 1 Part II Module (SAM)
- Minimum of 1 Part IV Module (PPM or approved alternative)
- One (1) additional module of [his] choice (Part II or Part IV)
- Completion of one hundred fifty (150) credits of acceptable CME (minimum 50% Division I), acquired in last three (3) years
- Compliance with ABFM Guidelines for Professionalism, Licensure, and Personal Conduct which includes holding a currently valid, full and unrestricted license to practice medicine in the United States or Canada
- Submission of three (3) MC-FP Process Payments; one (1) payment at the start of each module
- Submission of application and accompanying full examination fee for the MC-FP Examination
- Successful completion of the MC-FP Examination (Viewed April 23, 2013)
36. The foregoing requirements further impose many thousands of dollars in fees and travel expenses.
37. The foregoing requirements take physicians away from providing care for patients.
38. In addition, the ABMS has entered into agreements with many of the above-referenced 24 specialty organizations to require even more expenditures of time and money by physicians. According to an email sent to physicians by the American Board of Internal Medicine (ABIM) on or about April 6, 2013, Defendant “ABMS is requiring more frequent participation in MOC of all board certified physicians.”
39. Like many other AAPS physician members, J.E. spends a substantial percentage of his time providing charity care to patients who would not otherwise have access to medical care.
40. J.E. manages and works in a standalone medical charity clinic for a substantial part of each week.
41. Requiring J.E. to spend hundreds of hours on requirements for recertification under ABMS MOC® would result in an hour-for-hour reduction in his availability to provide medical care to his many charity patients, who recently surpassed 30,000 patient visits in total number.
42. Patients of J.E. typically lack any alternate means of obtaining comparable medical care.
43. J.E. continued to serve his charity patients rather than comply with the foregoing burdens of recertification demanded by Defendant’s agreement with ABFM to implement ABMS MOC®.
44. Effective June 24, 2011, SMC excluded J.E. from its medical staff, as a result of Defendant ABMS’s agreements with other entities to require the ABMS MOC® program.
45. Patients are now denied the benefit of being evaluated and treated by J.E. when taken by emergency to SMC.
46. There is no value to patients in the completion of the above litany of onerous recertification requirements.
47. The lack of any genuine value of ABMS MOC® as a measure of professional skill or competence is demonstrated (viewed March 4, 2013) by how ABMS itself selected and appointed as its new President/CEO in 2012 someone who was “Not Meeting MOC Requirements,” but had an exemption not available to younger physicians.
48. J.E. is unquestionably a first-rate physician who continues to practice in good standing in New Jersey.
49. Whether J.E. purchases and complies with ABMS MOC®, as implemented by the ABFM, has no bearing on his medical skills as a physician.
50. Like J.E., other members of AAPS face imminent injury from Defendant’s agreements to impose ABMS MOC®, and Defendant’s concerted actions to require physicians to purchase and comply with its proprietary product.
51. Defendant’s agreements and concerted actions limit the supply of physicians available to hospitalized patients, thereby denying patients care by their choice of physicians."
"Regarding opting out (from MOC®), I can demonstrate harm to my patients. As you know, I did not pay the $1300 to the ABP. I have no educational requirements due until 2023. Within weeks of not paying, Blue Cross/Blue Shield of Michigan (BCBSM) sent me a letter dated 19 January 2017 (and received by my office 28 Feb 2017) telling me to pay by 20 March, 2017 or I would be kicked off their panel. I mailed my appeal letter 1 March 2017. When I did not pay, BCBSM did not contact me to initiate the appeal process detailed in my contract ( which involves two peer-to-peer hearings where I can explain by case). Instead, they sent letters directly to my patients telling them I was no longer a qualified in-network physician and they would be reassigned to another doctor. I was not allowed to see my patients without having another physician in the room with me. Even if my patients decided to pay cash to see me, any prescriptions or studies ordered would not be covered by BCBSM. On March 10, 2017, I received notice that my appeal hearing was granted for 5 April 2017.As seen in these examples above, the American Board of Medical Specialties' MOC® program is not a benign recurrent educational exercise for physicians. Rather, MOC® is a means of assuring a continuous cash flow to ABMS member boards using threats and intimidation by unaccountable ABMS member board members and insurers that adversely affects patients as well.
They refused to stop sending the letters pending my active appeal case. They said they would continue sending letters until I complied, or my appeal was done, whichever happened first. Obviously, this caused extreme distress for my patients and my staff. I contacted a lawyer with the Michigan State Medical Society, who told me to pay the money. I did.
Within seconds I had my board certificate in hand. Within hours BCBS re-instated me and never sent out another letter. Of course, they never sent letters to the hundreds of patients letting them know of their error. I am not the only one this has happened to, it happens all the time. To opt out of MOC®, docs are hiring NPs to see their BCBS patients because they will credential a NP...but not a MD opting out of MOC®. It's madness that MOC® is now more important than a MD."
{kind=link}
- Wes
Tuesday, August 01, 2017
JAMA: The Certification Fees and Finances of US Medical Specialty Boards
Today in JAMA, a partial list of the fees and finances of the ABMS member boards were disclosed in a research letter to the editor from Brian C. Drolet, MD and Vickram J. Tandon, MD of the Departments of Plastic Surgery from Vanderbilt University and the University of Michigan. Their summary of those finances is remarkable:
Please consider joining Practicing Physicians of America, Inc. to help end the extortion of practicing US physicians by the ABMS specialty boards and their collaborating organizations at the Accreditation Council of Graduate Medical Education.
-Wes
Reference: Drolet BC and Tandon VJ. Fees for Certification and Finances of the Medical Specialty Boards. JAMA 1 Aug 2017; 218(5): 477-479.
Update: (video via MedPageToday) Where Do all Those MOC Fees Go?
StatNews: Medical Boards Ring Up Big Margins by Charging Doctors High Examination Fees
In total, the boards reported $701 million (85% CI, $644 million-$758 million) in assets and $65.6 million (95% CI, $60 million - $71 million) in liabilities (difference, $635 million (95% CI, $584 million - $687 million))(Table 2). Six boards reported no debt; and the remaining 18 held reported assets that substantially exceeded liabilities. Between 2003 and 2013, the change in net balance (ie, the difference of assets and liabilities) of the ABMS member boards grew from $237 million (85% CI, $232 million-241 million) to $635 million (95% CI, $584 million - $687 million). ... As a result of such margins, the member boards saw a mean annual growth rate of 10.4% during the decade studied.Importantly, these financial assets are significantly underreported. As the authors mentioned in their letter:
This study is limited by the data source. Although IRS Form 990s includes major funding sources and amounts of revenue, expenses, liabilities, and assets, it does not contain complete and specific financial accounting for the ABMS member boards. Also, board subsidiaries and foundations were not included. (Emphasis mine).Given these data, justification for Maintenenace of Certification for anything other than financial renumeration for the ABMS member boards and their supporting organizations is impossible to dispute. Their windfall is a direct result of the creation of Maintenance of Certification and their monopolization of the physician credentialing market by regulatory capture.
Please consider joining Practicing Physicians of America, Inc. to help end the extortion of practicing US physicians by the ABMS specialty boards and their collaborating organizations at the Accreditation Council of Graduate Medical Education.
-Wes
Reference: Drolet BC and Tandon VJ. Fees for Certification and Finances of the Medical Specialty Boards. JAMA 1 Aug 2017; 218(5): 477-479.
Update: (video via MedPageToday) Where Do all Those MOC Fees Go?
StatNews: Medical Boards Ring Up Big Margins by Charging Doctors High Examination Fees
Subscribe to:
Posts (Atom)