It has been a busy year for this blog and for doctors in general. While the number of posts have dwindled compared to my earlier experience in this space, I have enjoyed "diving deep" into topics with greater research behind them. Like others, I suspect my impact in the medical blog-o-sphere has been far more influential here than if I had stuck to a conventional medical journal format for publication of these topics. So far, 2015 promises to be no different.
So, for what it's worth, here are my most-read "top ten" blog posts of 2014:
10. The Effects of Maintenance of Certification and Crony Capitalism
9. Paid NEJM Subscriptions: There's No Such Thing As a Free Lunch
8. Reviewing the Regulators
7. The Importance of Demonizing Specialists
6. The New CMS National Coverage Decision for Pacemakers
5. The Business of Testing Physicians
4. For Medical Students, It Seems Nothing Has Changed
3. What Is Non-valvular Atrial Fibrillation?
2. How Much Do Doctors Really Earn? The public's interest in this topic seems insatiable.
1. The ABIM Foundation, Choosing Wisely, and the $2.3 Million Condominium The grand-daddy of them all, with already over 17,100 page views as of today and just posted a little over a week ago.
Yes, I'd say it's been a very productive year indeed.
-Wes
Sunday, December 28, 2014
Wednesday, December 24, 2014
Merry Christmas to All
To every person who finds themselves sick or alone this holiday season. To the many caregivers who toil without recognition this day and the next. May the peace and joy of this holiday season transcend it all as we pause and reflect on what really matters.

Merry Christmas and Happy Holidays to all.
-Wes
Merry Christmas and Happy Holidays to all.
-Wes
Monday, December 22, 2014
Medical Journals Should Disclose Conflicts Just Like Their Authors
In every medical journal, authors must disclose all conflict of interests that might exist to the editors of that journal as a condition of publication. However, as we are increasingly becoming aware, journal editors do not have to disclose payments they receive from outside sources (pharmaceutical industry, special interests, the government) to publish content in their own journal. I think they should.
Medical journals, especially those with large physician "reach," are being used less for scientific endeavors and more for political or marketing agendas. Of course, this is nothing new, in medicine, but it's high time medical journals understand that with the availability of information on the internet, that "special arrangements" with various entities might not remain so private any longer. As I noted in my earlier blog post regarding the simultaneous publication of a non-peer reviewed white paper in the Annals of Internal Medicine and The Lancet and this publication's association to recent revelations concerning the finances of the American Board of Internal Medicine and their Foundation, such a practice risks jeopardizing their scientific credibility, especially if those revelations are found to be credible. Legitimacy is an important asset to medical journals and medical journal editors should be aware that physicians who are increasingly being subject to political agendas are growing increasingly frustrated at this covert practice.
More recently, we've seen the editorial decision of another medical journal, the Journal of the American Medical Association (JAMA), decide to allow the conflict of interests of choosing Press Ganey Chief Medical Officer Thomas H Lee, MD as an editorial author for a discussion surrounding the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) in their 10 Dec 2014 issue. Also, the fact that pointed questions to a webcast supporting the ABIM's MOC process had many questions cherry-picked by the moderators. I have no problem with a journal siding with one opinion or the other provided there is full disclosure about the financial relationships of the authors of the paper AND those of the journal itself. But any legitimate discussion requires the disclosure of real or potential conflicts of interests held by the journal to critically review the credibility of what is published. Any double-standard regarding the disclosure of conflicts of interest should not be tolerated by the medical community, especially by physicians who struggle to improve the care of our patients in our evolving health care system, especially when that health care system appears to be increasingly hostile toward physicians and their patients.
-Wes
Medical journals, especially those with large physician "reach," are being used less for scientific endeavors and more for political or marketing agendas. Of course, this is nothing new, in medicine, but it's high time medical journals understand that with the availability of information on the internet, that "special arrangements" with various entities might not remain so private any longer. As I noted in my earlier blog post regarding the simultaneous publication of a non-peer reviewed white paper in the Annals of Internal Medicine and The Lancet and this publication's association to recent revelations concerning the finances of the American Board of Internal Medicine and their Foundation, such a practice risks jeopardizing their scientific credibility, especially if those revelations are found to be credible. Legitimacy is an important asset to medical journals and medical journal editors should be aware that physicians who are increasingly being subject to political agendas are growing increasingly frustrated at this covert practice.
More recently, we've seen the editorial decision of another medical journal, the Journal of the American Medical Association (JAMA), decide to allow the conflict of interests of choosing Press Ganey Chief Medical Officer Thomas H Lee, MD as an editorial author for a discussion surrounding the American Board of Internal Medicine (ABIM) Maintenance of Certification (MOC) in their 10 Dec 2014 issue. Also, the fact that pointed questions to a webcast supporting the ABIM's MOC process had many questions cherry-picked by the moderators. I have no problem with a journal siding with one opinion or the other provided there is full disclosure about the financial relationships of the authors of the paper AND those of the journal itself. But any legitimate discussion requires the disclosure of real or potential conflicts of interests held by the journal to critically review the credibility of what is published. Any double-standard regarding the disclosure of conflicts of interest should not be tolerated by the medical community, especially by physicians who struggle to improve the care of our patients in our evolving health care system, especially when that health care system appears to be increasingly hostile toward physicians and their patients.
-Wes
Tuesday, December 16, 2014
The ABIM Foundation, Choosing Wisely®, and the $2.3 Million Condominium
Is it "medically professional" for a non-profit organization to use
physician testing fees to "choose wisely" a $2.3 million luxury
condominium complete with a chauffeur-driven BMW 7-series town car? In my view, obviously not. To most people such an action would conjure up images of hypocrisy, waste, and
corruption.
Yet, after a review of public and tax records, it appears to me this is exactly what has happened.
Background
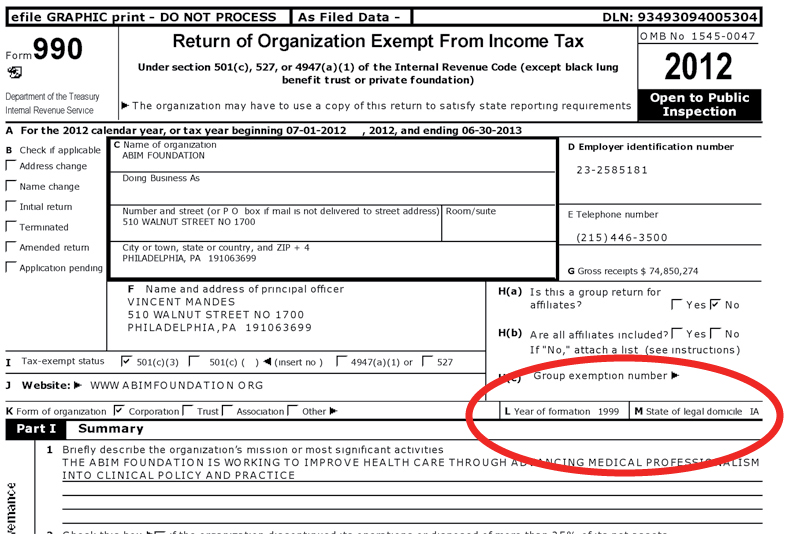
In 1999 for reasons that are unclear, the American Board of Internal Medicine (ABIM), itself a tax-exempt 501 (c) (3) independent non-profit physician evaluation organization domiciled in Iowa, created (Editor's note 10/20/2015: referenced web page has since been edited by the ABIM Foundation; the original referenced web page can be viewed here) a second non-profit tax-exempt 501 (c) (3) organization, the ABIM Foundation (Foundation), to first define and later promote the term "medical professionalism." Both the ABIM and the Foundation share a common address in Pennsylvania and common officers:
Ten years later after accumulating some $76 million in assets, the Foundation began their hard-to-disagree-with "Choosing Wisely®" campaign to encourage physicians and providers to question the value of medical testing in an effort to eliminate unnecessary tests and procedures. The campaign has grown to include 70 societies and some non-physician organizations, including Consumer Reports, AARP, SEIU, and Univision among others. As part of the campaign, monetary grants from the Robert Wood Johnson Foundation are awarded to institutions willing to "educate practicing physicians about the recommendations from specialty societies, and building physician communication skills to facilitate conversations with their patients about the care they need."
The Money Trail
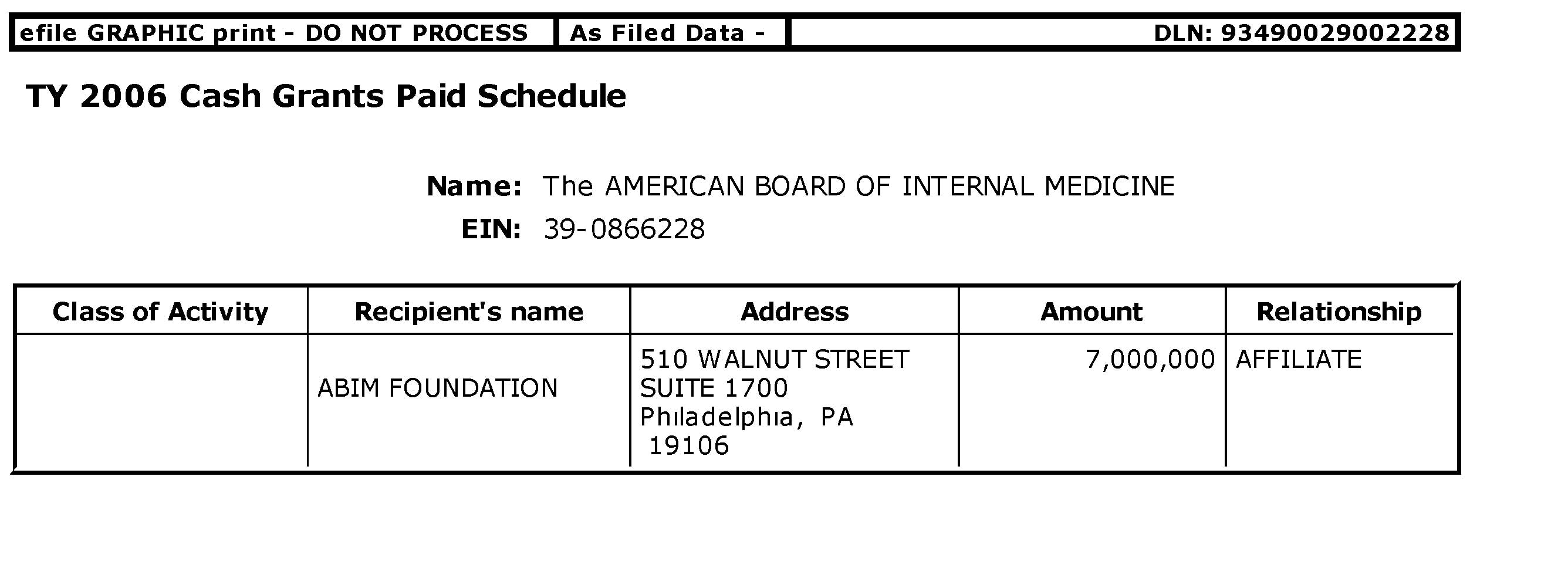
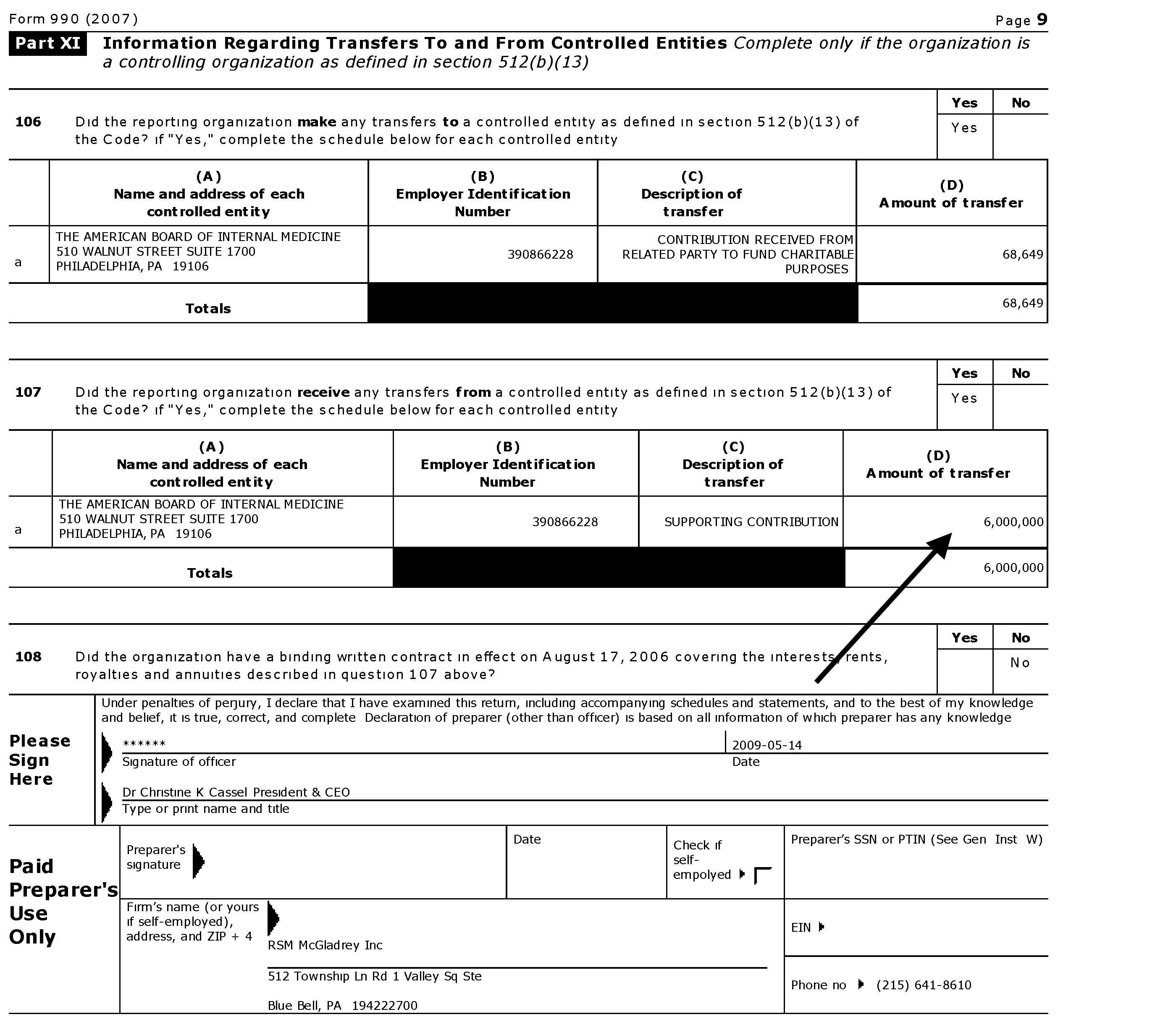
So how did the ABIM Foundation accumulate all that money? Reviewing public tax records of the ABIM and its Foundation reveals a significant portion of the Foundation's revenues came directly from the ABIM. Recall that ABIM receives 97% of its annual revenues from physician certification (62%) and re-certification fees (35%), with only 14% of these fees going toward physician examination development. In 2007 and 2008 alone, cash grants from the ABIM to its Foundation of $7 million and $6 million respectively were issued. The public records disclosed that $17,360,000 from the ABIM were made to its Foundation in the 7 years ending 6/30/2008. As a three-time participant in the ABIM certification process (candidate #127308), I can attest that to the best of my knowledge physicians were never made aware of this use of the testing fees they paid the ABIM.
The Luxury Condominium
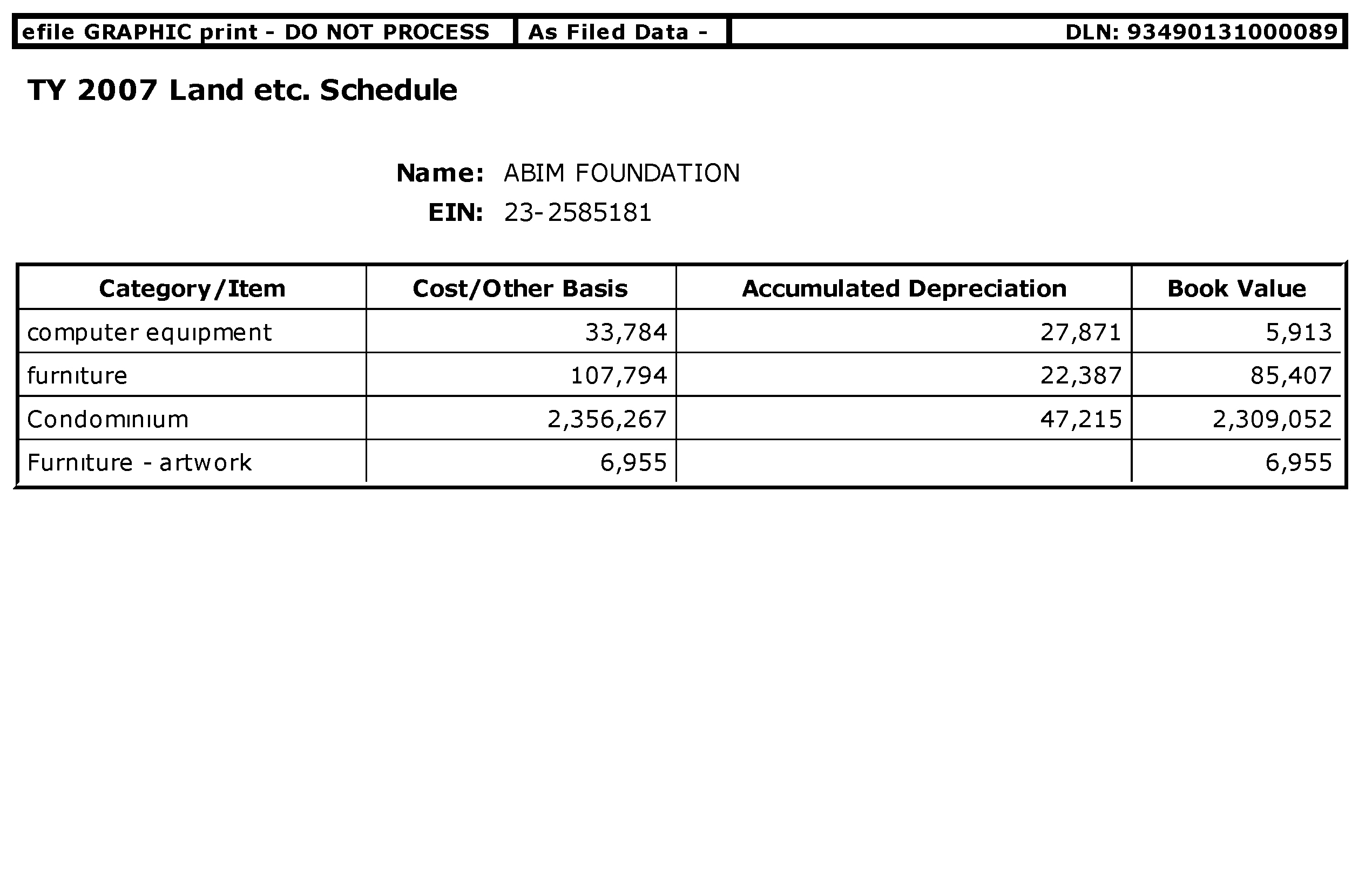
So why did the ABIM Foundation need all this cash from physicians? We can't be certain, but the Foundation disclosed in their 2008 Form 990 that a portion of the
money they received from the ABIM via physicians fees was used to purchase a 2,579 square foot 3-bedroom luxury
condominium (Unit #11NW, in the "Ayer" Building, 210 W. Washington Square, Philadelphia) in December 2007 for $2.3 million. The luxury property borders Washington Square Park of the most historic areas of Philadelphia, across the street from the Tomb of the Unknown Revolutionary War Soldier and the Eternal Flame. The condominium building previously advertised a chauffeur driven Mercedes Benz S-series town car (more pictures here).
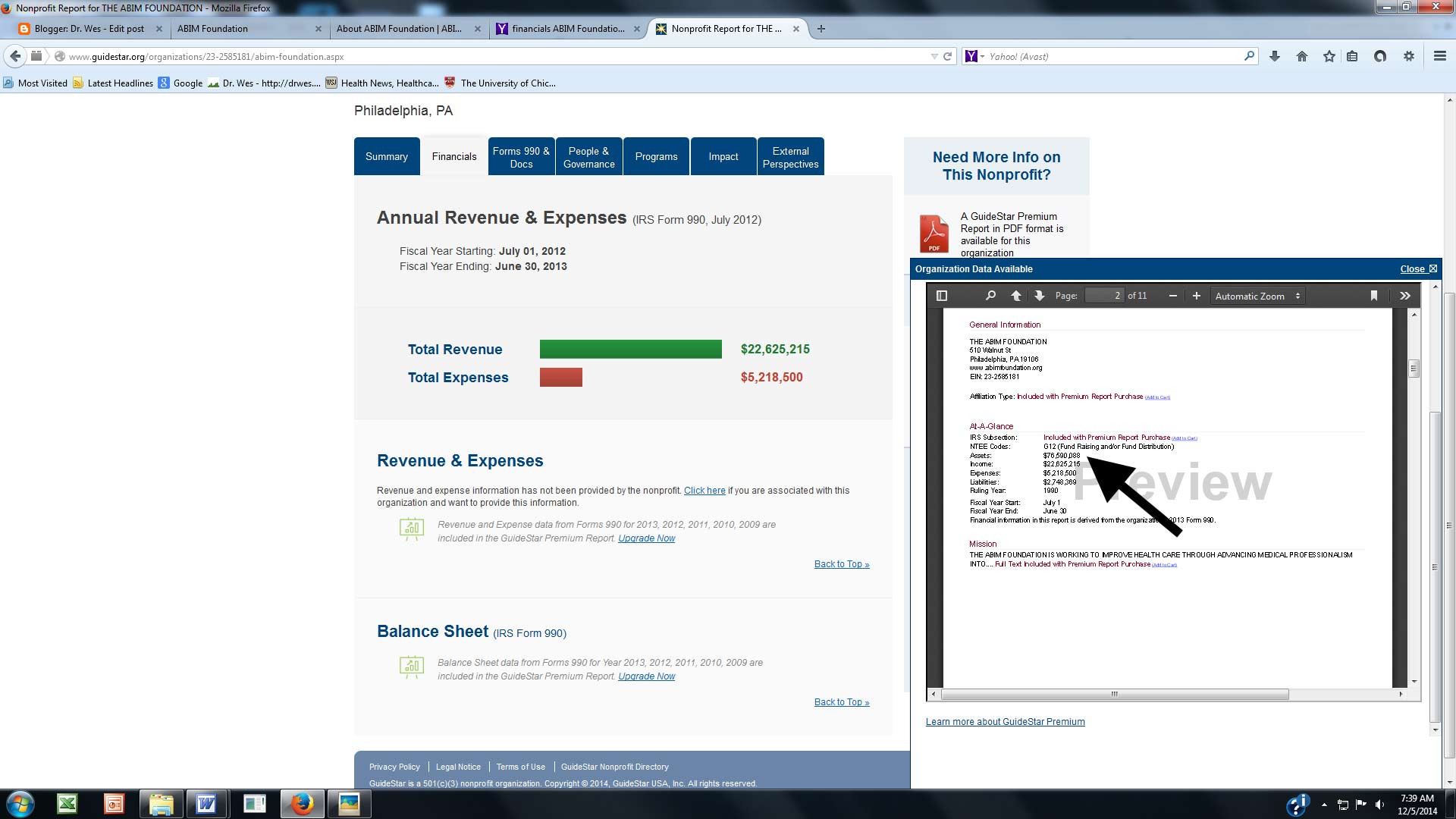
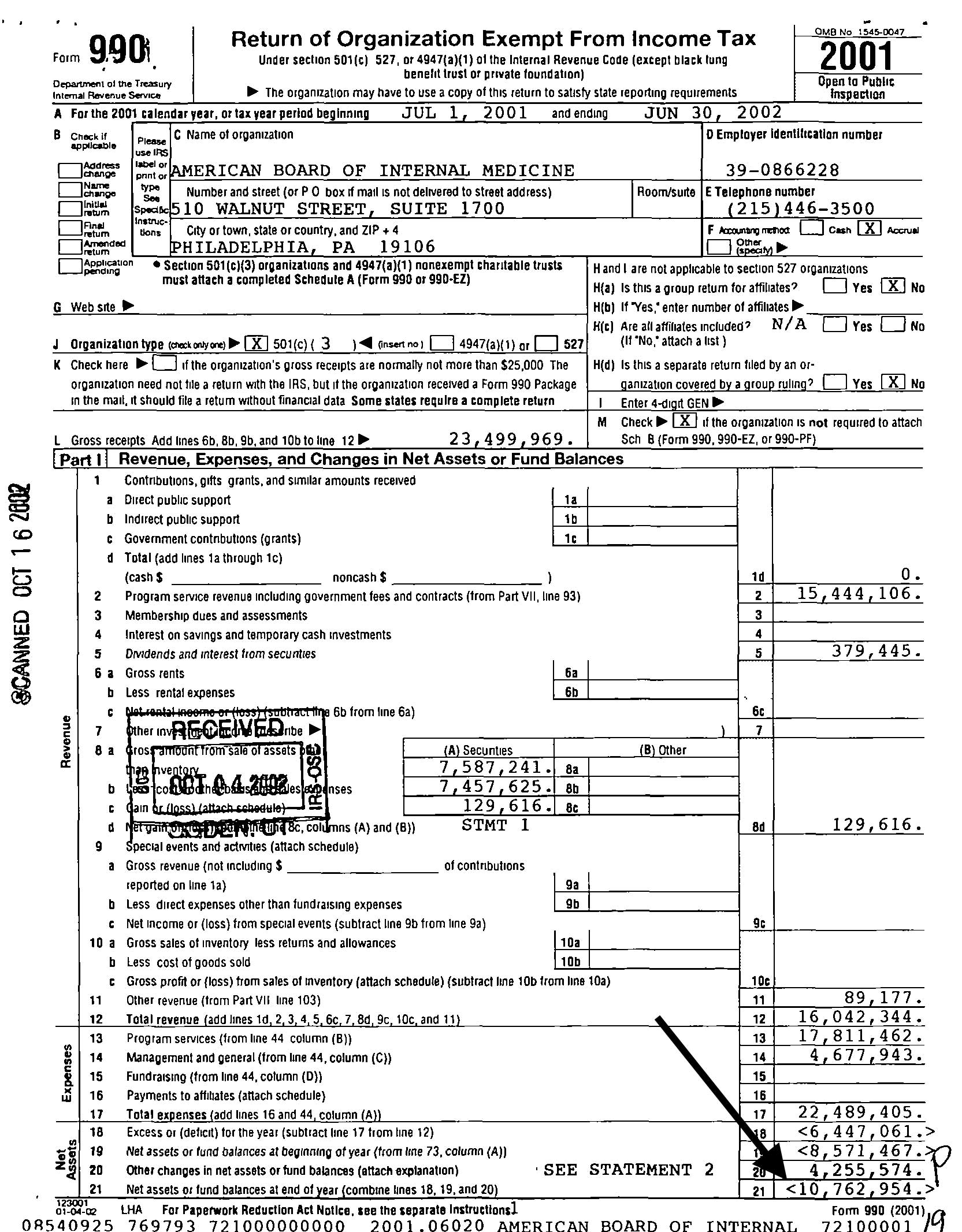
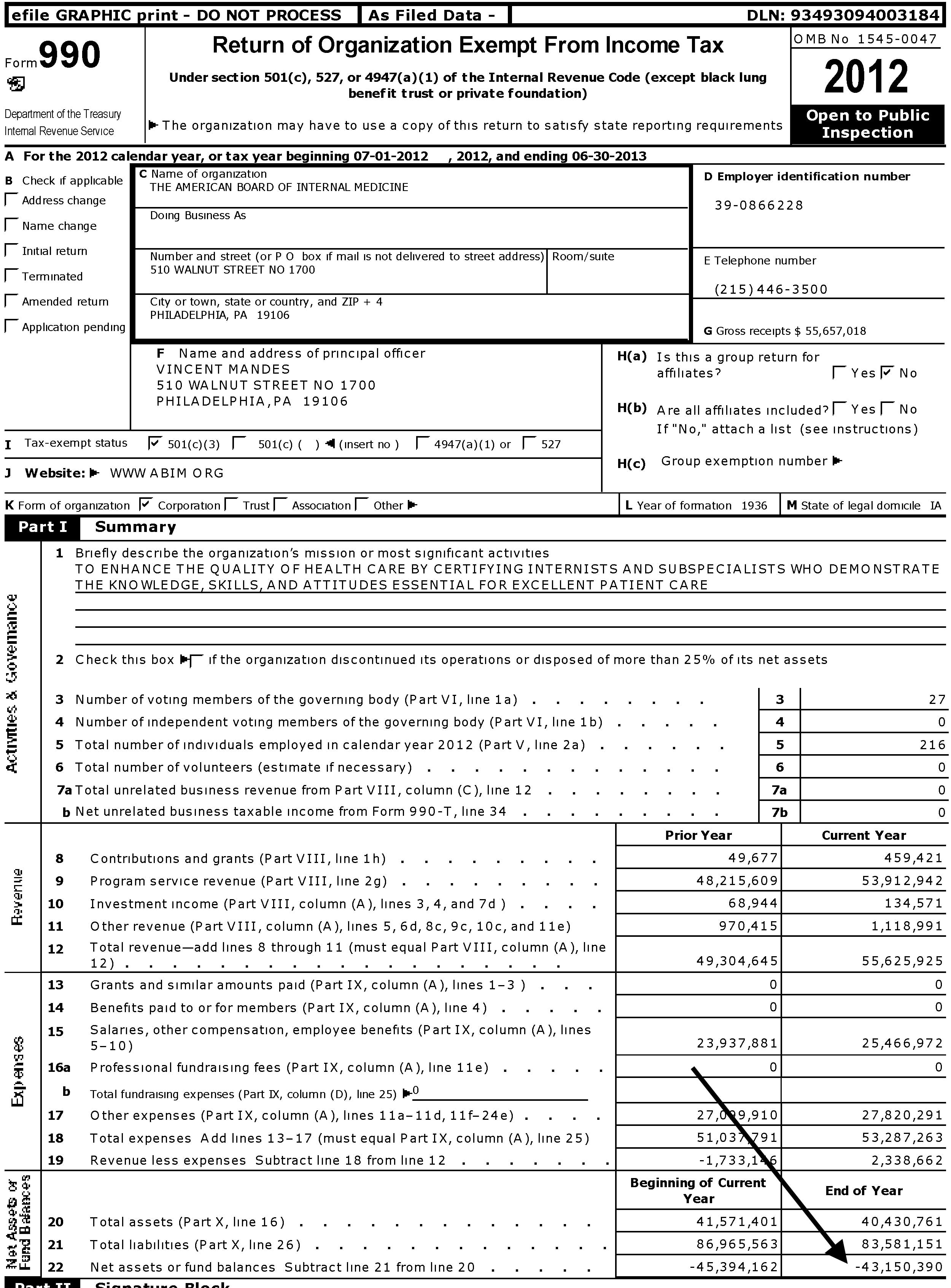
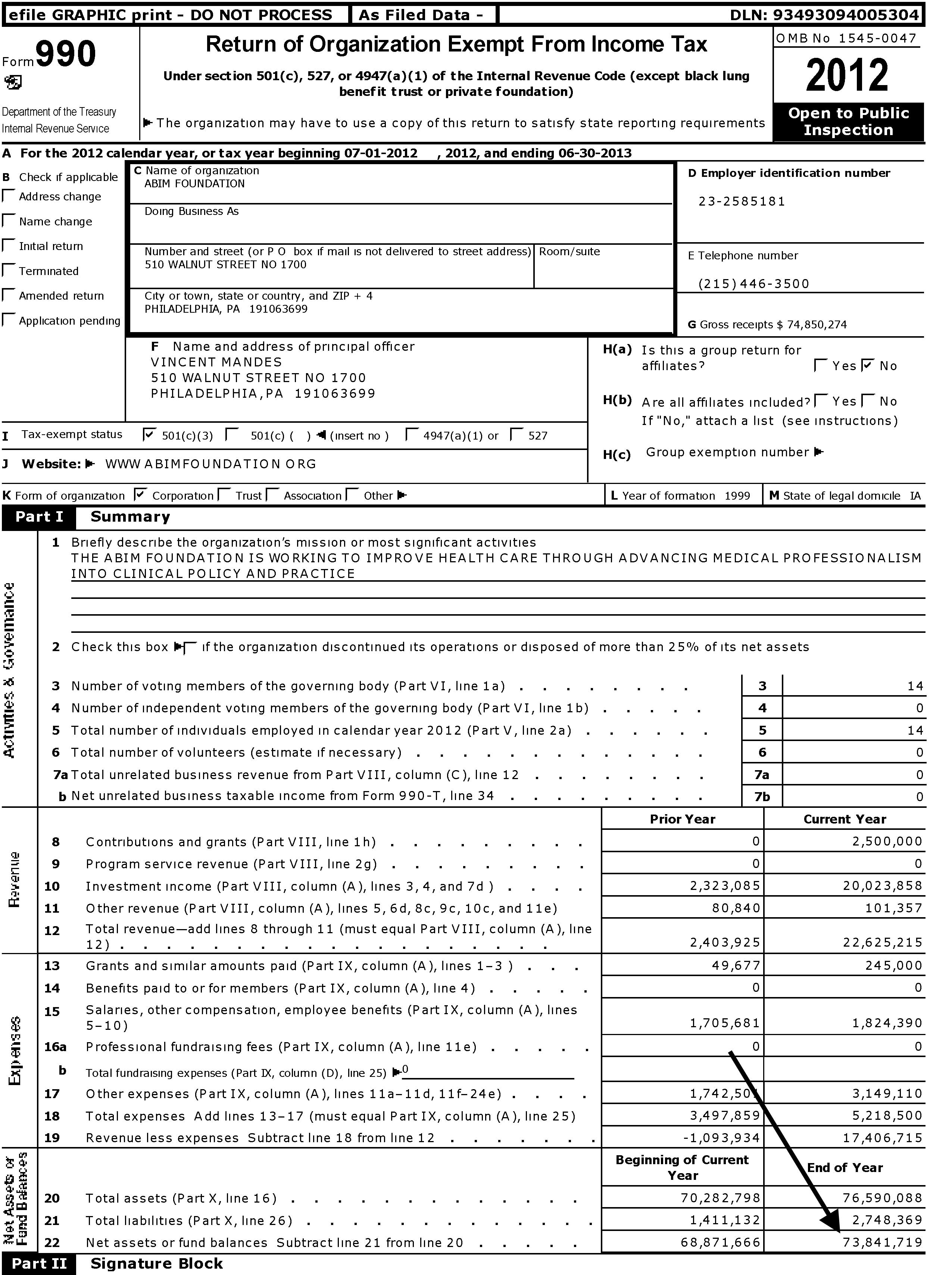
Since then, the Foundation has reported "condominium expenses" totaling $850,340 from December 2007 through June 30, 2013 (FY 2008: $42,522, FY 2009: $164,460, FY 2010: 161,957, FY 2011: $165,982, FY 2012: $161,980, FY 2013: $153,439 (most of these reported as "program service expenses")). In my view, these expenses were accrued while the ABIM appears to have been on an inherently unsustainable financial course from 2001 to 2012 with its net asset or fund balances on 6/30/2002 beginning with a negative balance of $10,762,954 and growing to a negative balance of $43,150,390 ending 6/30/2013. Meanwhile, over the same period its shadow organization, the ABIM Foundation, fund balance was $73,841,719 on 6/30/2013.
It should be noted that in the year of the condominium purchase the President and CEO of the ABIM, Christine Cassel, MD, earned $484,883 from the ABIM and $161,627 from the Foundation. Dr. Cassel continues to serve as President and CEO of the National Quality Forum despite a history of other seemingly conflicted financial dealings. Other executives of ABIM that year included F. Daniel Duffy, MD who served as Executive Vice President of the ABIM earning $379,915 from the ABIM, and Cary Sennett, MD, PhD who served as Senior Vice President earning $185,122 from the ABIM and $185,122 from the Foundation and now serves as a Vice President of Anthem, Inc., formerly Wellpoint. That year Dr. Richard Baron, the current President and CEO of the ABIM and Foundation, served as the secretary/treasurer of the ABIM Board earning $59,729 until 7/1/2008 when he became an unpaid Director of the Board. By comparison, according to one reliable source, the median general internal medicine physician salary in the U.S. was $205,441 in 2009.
More Questions
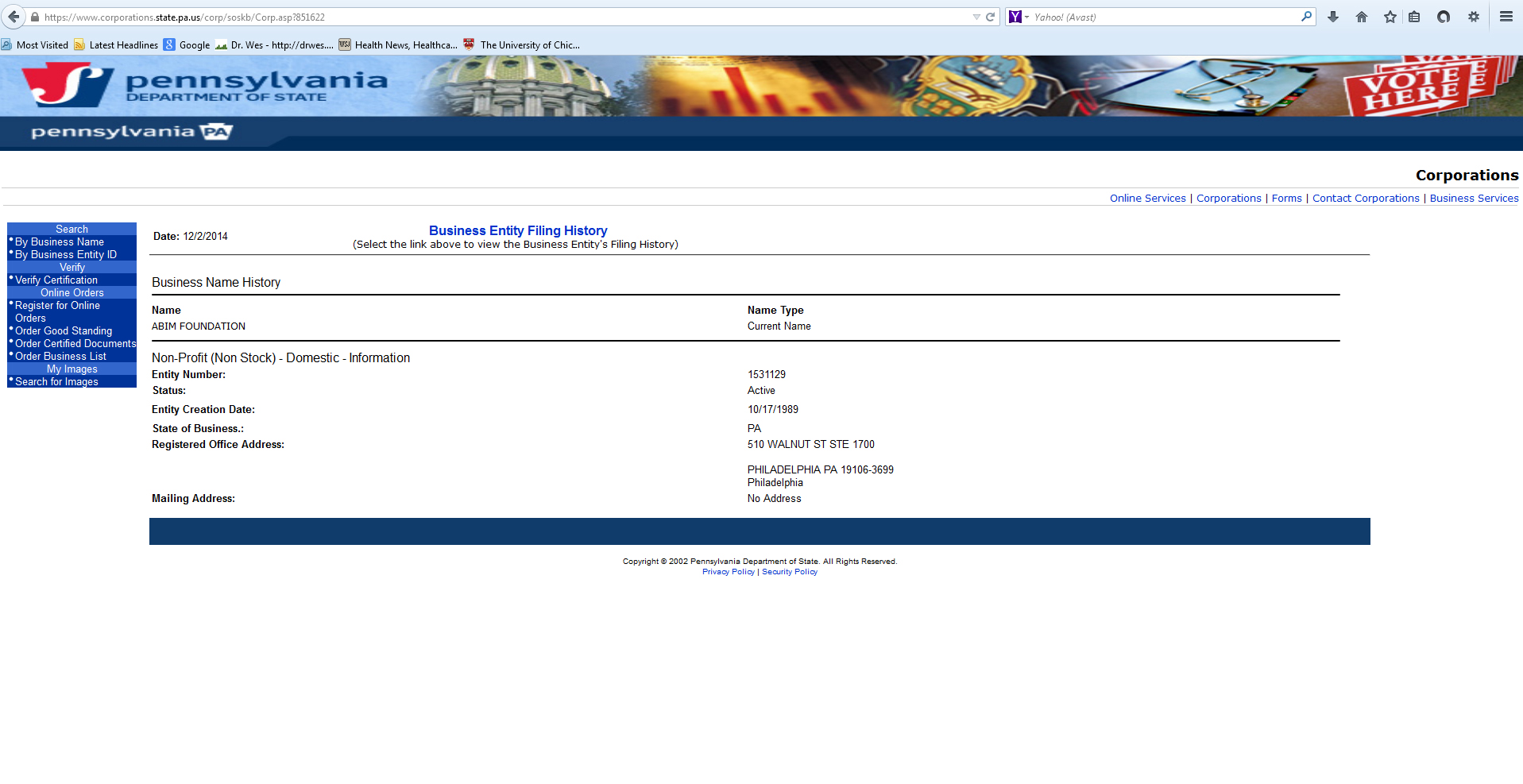
Reviewing the public record on when and where the ABIM Foundation was actually created discloses another discrepancy. We observe that the Foundation has recorded on their tax returns as being founded in 1999 with its "legal domicile" in Iowa, like the ABIM. However, a search for the organization in Iowa comes up empty, while a search in Pennsylvania Department of State (screen shot here) shows the Foundation was actually created in Pennsylvania in 1989. Which is correct?
We should note that non-profits are not required to file financial statements with the state of Iowa, while Pennsylvania requires them. This raises uncomfortable questions. Is the Foundation's Iowa domicile sheltering the sources and uses of its funds? Why does a non-profit promoting "medical professionalism" need to accumulate this much revenue? Is this how the Foundation demonstrates their "medical professionalism" to the public? To whom is the ABIM and Foundation "accountable?" Anyone?
My Call to the ABIM
On 4 December 2014 I contacted the ABIM and requested an explanation regarding the condominium, the ongoing condominium expenses, and the discrepancy of the ABIM Foundation domicile and founding date. Richard Baron, MD, the current President and CEO of the ABIM returned my call and explained the following:
Larger Implications
Sadly, the medical profession has become a house divided. On one side are many non-clinical physicians who have become far removed from patient care and are firmly embedded in the non-profit, academic, and public policy circles making handsome salaries while seeing little problem with coercing their colleagues to pay fees to support their various economic, policy, or personal agendas. In the words of my colleague Jordan Grumet, MD: "they talk about 'accountability' as if they are the ones in the ICU having the family meetings. They pray at the altar of 'quality' yet fail to define the specifics of such a term. They resent 'over treatment' but never have suffered the consequences of not doing enough."
On the other side are the physicians buried in the work-a-day world of patient care, busy doing the best they can for their patients in our increasingly complicated health care system, working as "excellent sheep" as they do their difficult job and try not to rock the boat. While such a dichotomy is not unique to medicine (look to education, the public service sector, and politics, for instance), is ignoring this new reality useful to our profession? Might the unintended consequences of these unaccountable non-profit organizations and revolving-door employment practices with government and business interests be causing unimaginable harm to the integrity and credibility of our profession while simultaneously wasting valuable resources?
It is a shame that most physicians, particularly younger doctors saddled with exorbitant training debt and concerns of job acquisition and job security, are not in a position to protest the actions of the ABIM and its sycophants, particularly since their ability to practice medicine is increasingly tied to these ABIM board certification and their new perpetual maintenance of certification payments. But this is the point, isn't it? Regulatory capture. As these younger doctors gain experience and awaken to the realities of their new health care arena that is increasingly dominated by unaccountable organizations led by non-clinical members of our own profession, we risk creating cynicism in our ranks and physicians who must be more concerned with passing a test than providing direct patient care. Even worse, we risk promoting ourselves, career or cause over the complicated needs of our patients as the divide grows ever deeper. As a result, the brittle credibility and hard-earned trust with our patients is squandered beyond repair. In my opinion, this is what we risk when we have corruption within.
Is this what our profession and the public wants?
I can only hope that practicing US physicians and the public will demand a full accounting of the ABIM and their Foundation's entire financial dealings and non-transparent co-mingling of funds. I hope that Congress decides to investigate the ABIM's role in including their MOC program as a physician quality reporting measure in the Affordable Care Act (see pages 247 and 844-845) to determine its legitimacy in light of these findings. Furthermore, an investigation into possible violations of federal policy on the protection of human subjects (in this case practicing physicians involved in direct patient care) regarding the American Board of Medical Specialties' requirement for practice and patient survey collection for Part IV of their trademarked Maintenance of Certification® program that the ABIM helps conduct should occur, especially in light of lack of informed consent afforded to physicians regarding how the fees and data they collect are used.
It is time we hold the non-clinical members of our own profession that lead these organizations accountable to all physicians and the public at large. Until this occurs, physician-members of every ABIM subspecialty organization that profits from educational content provided to the ABIM should divest themselves and work to create their own, more credible, simplified and transparent life-long learning pathways. The American Association of Clinical Endocrinologists has already set a good example. While I understand that refusing to buck the coercion created by the multimillion dollar ABIM and its Foundation will be difficult, our credibility as stewards of our patients' best interests and the preservation of the integrity of our profession demands nothing less.
-Wes
Acknowledgement
I am indebted to Charles P. Kroll, CPA for his invaluable assistance collecting tax records of the ABIM and ABIM Foundation before 2007 and assisting in the understanding of the nuances of not-for-profit accounting methods. Mr. Kroll provided forensic accounting analysis to the Minnesota attorney general's office during the Medica-Allina scandal and testified at the Minnesota Senate hearing on the matter.
Yet, after a review of public and tax records, it appears to me this is exactly what has happened.
Background
In 1999 for reasons that are unclear, the American Board of Internal Medicine (ABIM), itself a tax-exempt 501 (c) (3) independent non-profit physician evaluation organization domiciled in Iowa, created (Editor's note 10/20/2015: referenced web page has since been edited by the ABIM Foundation; the original referenced web page can be viewed here) a second non-profit tax-exempt 501 (c) (3) organization, the ABIM Foundation (Foundation), to first define and later promote the term "medical professionalism." Both the ABIM and the Foundation share a common address in Pennsylvania and common officers:
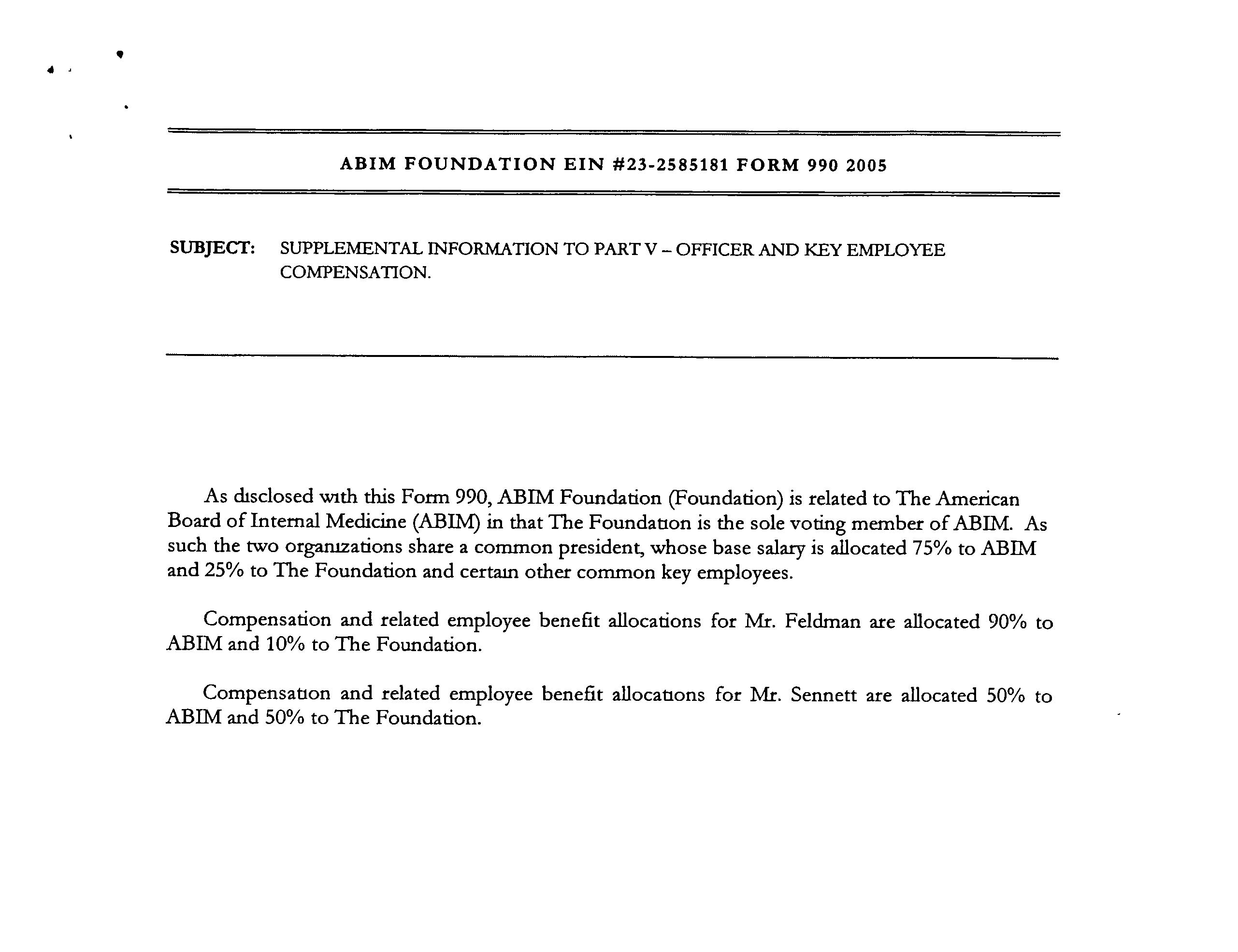{kind=link}
"The American Board of Internal Medicine (ABIM) is related to the ABIM Foundation (Foundation) in that The Foundation is the sole voting member of the ABIM. As such, the two organizations share a common president, a common CFO, and a common senior vice president whose base salaries are allocated between ABIM and The Foundation based on the time spent by each executive."To define "medical professionalism," the new Foundation enlisted other members of the non-profit world including the ABIM, the paid "directors" of the Foundation, the Robert Wood Johnson Foundation, the American College of Physicians-American Society of Internal Medicine and the European Federation of Internal Medicine. The group was chaired by Troy Brennan, MD, JD a paid "Director" of the Foundation who was also President and CEO of Brigham and Women's Physician Organization at the time. (He later became the Chief Medical Officer of Aetna in 2006, and now serves as the Executive Vice President and Chief Medical Officer of CVS Caremark). In 2002 this group published a white paper entitled "Medical Professionalism in the New Millenium: A Physician Charter" without peer review in the Annals of Internal Medicine (here) and The Lancet (here). At least the Annals editor, Harold C. Sox, MD mustered the courage to express concerns about the manuscript in his introductory remarks to his readers:
"The introduction contains the following premise: Changes in the health care delivery systems in countries throughout the industrialized world threaten the values of professionalism. The document conveys this message with chilling brevity. The authors apparently feel no need to defend this premise, perhaps because they believe that it is a universally held truth. The authors go further, stating that the conditions of medical practice are tempting physicians to abandon their commitment to the primacy of patient welfare. These are very strong words. Whether they are strictly true for the profession as a whole is almost beside the point. Each physician must decide if the circumstances of practice are threatening his or her adherence to the values that the medical profession has held dear for many millennia."The paper centered on three fundamental principles that the authors claimed defined "medical professionalism:" (1) the primacy of patient welfare, (2) patient autonomy, and a new concept, (3) the principle of social justice - that is, "the medical profession must promote justice in the health care system, including the fair distribution of health care resources." With this definition, physicians could no longer just be unwavering patient advocates concerned with the "primacy of their patient's welfare," they had also had to serve the financial needs of The System of medicine lest they be labeled "medically unprofessional."
Ten years later after accumulating some $76 million in assets, the Foundation began their hard-to-disagree-with "Choosing Wisely®" campaign to encourage physicians and providers to question the value of medical testing in an effort to eliminate unnecessary tests and procedures. The campaign has grown to include 70 societies and some non-physician organizations, including Consumer Reports, AARP, SEIU, and Univision among others. As part of the campaign, monetary grants from the Robert Wood Johnson Foundation are awarded to institutions willing to "educate practicing physicians about the recommendations from specialty societies, and building physician communication skills to facilitate conversations with their patients about the care they need."
{kind=link}
The Money Trail
So how did the ABIM Foundation accumulate all that money? Reviewing public tax records of the ABIM and its Foundation reveals a significant portion of the Foundation's revenues came directly from the ABIM. Recall that ABIM receives 97% of its annual revenues from physician certification (62%) and re-certification fees (35%), with only 14% of these fees going toward physician examination development. In 2007 and 2008 alone, cash grants from the ABIM to its Foundation of $7 million and $6 million respectively were issued. The public records disclosed that $17,360,000 from the ABIM were made to its Foundation in the 7 years ending 6/30/2008. As a three-time participant in the ABIM certification process (candidate #127308), I can attest that to the best of my knowledge physicians were never made aware of this use of the testing fees they paid the ABIM.
{kind=link}
{kind=link}
The Luxury Condominium
 |
| Street View, "The Ayer Buidling," 210 W. Washington Square |
{kind=link}
Since then, the Foundation has reported "condominium expenses" totaling $850,340 from December 2007 through June 30, 2013 (FY 2008: $42,522, FY 2009: $164,460, FY 2010: 161,957, FY 2011: $165,982, FY 2012: $161,980, FY 2013: $153,439 (most of these reported as "program service expenses")). In my view, these expenses were accrued while the ABIM appears to have been on an inherently unsustainable financial course from 2001 to 2012 with its net asset or fund balances on 6/30/2002 beginning with a negative balance of $10,762,954 and growing to a negative balance of $43,150,390 ending 6/30/2013. Meanwhile, over the same period its shadow organization, the ABIM Foundation, fund balance was $73,841,719 on 6/30/2013.
{kind=link}
{kind=link}
{kind=link}
It should be noted that in the year of the condominium purchase the President and CEO of the ABIM, Christine Cassel, MD, earned $484,883 from the ABIM and $161,627 from the Foundation. Dr. Cassel continues to serve as President and CEO of the National Quality Forum despite a history of other seemingly conflicted financial dealings. Other executives of ABIM that year included F. Daniel Duffy, MD who served as Executive Vice President of the ABIM earning $379,915 from the ABIM, and Cary Sennett, MD, PhD who served as Senior Vice President earning $185,122 from the ABIM and $185,122 from the Foundation and now serves as a Vice President of Anthem, Inc., formerly Wellpoint. That year Dr. Richard Baron, the current President and CEO of the ABIM and Foundation, served as the secretary/treasurer of the ABIM Board earning $59,729 until 7/1/2008 when he became an unpaid Director of the Board. By comparison, according to one reliable source, the median general internal medicine physician salary in the U.S. was $205,441 in 2009.
More Questions
Reviewing the public record on when and where the ABIM Foundation was actually created discloses another discrepancy. We observe that the Foundation has recorded on their tax returns as being founded in 1999 with its "legal domicile" in Iowa, like the ABIM. However, a search for the organization in Iowa comes up empty, while a search in Pennsylvania Department of State (screen shot here) shows the Foundation was actually created in Pennsylvania in 1989. Which is correct?
{kind=link}
{kind=link}
We should note that non-profits are not required to file financial statements with the state of Iowa, while Pennsylvania requires them. This raises uncomfortable questions. Is the Foundation's Iowa domicile sheltering the sources and uses of its funds? Why does a non-profit promoting "medical professionalism" need to accumulate this much revenue? Is this how the Foundation demonstrates their "medical professionalism" to the public? To whom is the ABIM and Foundation "accountable?" Anyone?
My Call to the ABIM
On 4 December 2014 I contacted the ABIM and requested an explanation regarding the condominium, the ongoing condominium expenses, and the discrepancy of the ABIM Foundation domicile and founding date. Richard Baron, MD, the current President and CEO of the ABIM returned my call and explained the following:
- Dr. Baron stated that the condominium was purchased as a "investment property" and part of the investment portfolio of the Foundation. He mentioned that real estate holdings were not uncommon with other similar non-profits. The condominium was used for several purposes, including housing ABIM personnel who resided out of state and returned to Philadelphia for meetings, by contractors (for instance, to house an IT team from India), and for off-site retreats and meetings with the Communications Group of the ABIM, for instance. He noted that when ABIM members use the Foundation's condominium, the Foundation is paid $150/night from the ABIM (compared to the "usual" Philadelphia hotel rate of about $190/night) and there was cash flow to the Foundation from the ABIM for the use of their facility.
- After revelations of the luxury condominium were disclosed at a 2 Dec 2014 Pennsylvania Medical Society town hall meeting, Dr. Baron mentioned in passing that the ABIM was putting the condominium up for sale. I asked Dr. Baron the name of the listing agent and the price. He stated he could not comment because "the paperwork was not in order" and the those details had not been finalized because they were advised that the real estate market would be better in the Spring.
- When asked about the high ongoing condominium expenses and the discrepancy about the ABIM Foundation's creation date and domicile, Dr. Baron could not immediately respond but sent this follow-up e-mail 4 Dec 2014 at 2:39PM (CST):
"Hi Dr. Fischer (sic)-
Attached please find the breakdown of the condo expenses. As I explained the depreciation $$ are a required reporting artifact for the condo as a business investment. The other costs are covered by the condo usage fees.
Regarding the 1989/1999 question - In 1999 ABIM Foundation became a separate operating foundation.
Thanks,
Rich
Richard J. Baron, MD
MACP
President and Chief Executive Officer
American Board of Internal Medicine" - In closing, Dr. Baron expressed his willingness to be open to further questions.
- Today I learned that the condominium is now listed with the following description:
"Extremely Spacious Three Bedroom, 3.5 Bath Home at the Ayer Condominium. Tremendous Entertaining Space. 11’7’’ ceiling heights. Bulthaup b-3 kitchen system, Miele and Subzero Appliances. Huge windows with northwest views. High floor offering stupendous sunsets. Gorgeous stone bathrooms. Abundant closet space. One garage parking space included. Concierge, doormen, valets, gym, chauffeur driven BMW 7-Series." (More details here.)
Larger Implications
Sadly, the medical profession has become a house divided. On one side are many non-clinical physicians who have become far removed from patient care and are firmly embedded in the non-profit, academic, and public policy circles making handsome salaries while seeing little problem with coercing their colleagues to pay fees to support their various economic, policy, or personal agendas. In the words of my colleague Jordan Grumet, MD: "they talk about 'accountability' as if they are the ones in the ICU having the family meetings. They pray at the altar of 'quality' yet fail to define the specifics of such a term. They resent 'over treatment' but never have suffered the consequences of not doing enough."
On the other side are the physicians buried in the work-a-day world of patient care, busy doing the best they can for their patients in our increasingly complicated health care system, working as "excellent sheep" as they do their difficult job and try not to rock the boat. While such a dichotomy is not unique to medicine (look to education, the public service sector, and politics, for instance), is ignoring this new reality useful to our profession? Might the unintended consequences of these unaccountable non-profit organizations and revolving-door employment practices with government and business interests be causing unimaginable harm to the integrity and credibility of our profession while simultaneously wasting valuable resources?
It is a shame that most physicians, particularly younger doctors saddled with exorbitant training debt and concerns of job acquisition and job security, are not in a position to protest the actions of the ABIM and its sycophants, particularly since their ability to practice medicine is increasingly tied to these ABIM board certification and their new perpetual maintenance of certification payments. But this is the point, isn't it? Regulatory capture. As these younger doctors gain experience and awaken to the realities of their new health care arena that is increasingly dominated by unaccountable organizations led by non-clinical members of our own profession, we risk creating cynicism in our ranks and physicians who must be more concerned with passing a test than providing direct patient care. Even worse, we risk promoting ourselves, career or cause over the complicated needs of our patients as the divide grows ever deeper. As a result, the brittle credibility and hard-earned trust with our patients is squandered beyond repair. In my opinion, this is what we risk when we have corruption within.
Is this what our profession and the public wants?
I can only hope that practicing US physicians and the public will demand a full accounting of the ABIM and their Foundation's entire financial dealings and non-transparent co-mingling of funds. I hope that Congress decides to investigate the ABIM's role in including their MOC program as a physician quality reporting measure in the Affordable Care Act (see pages 247 and 844-845) to determine its legitimacy in light of these findings. Furthermore, an investigation into possible violations of federal policy on the protection of human subjects (in this case practicing physicians involved in direct patient care) regarding the American Board of Medical Specialties' requirement for practice and patient survey collection for Part IV of their trademarked Maintenance of Certification® program that the ABIM helps conduct should occur, especially in light of lack of informed consent afforded to physicians regarding how the fees and data they collect are used.
It is time we hold the non-clinical members of our own profession that lead these organizations accountable to all physicians and the public at large. Until this occurs, physician-members of every ABIM subspecialty organization that profits from educational content provided to the ABIM should divest themselves and work to create their own, more credible, simplified and transparent life-long learning pathways. The American Association of Clinical Endocrinologists has already set a good example. While I understand that refusing to buck the coercion created by the multimillion dollar ABIM and its Foundation will be difficult, our credibility as stewards of our patients' best interests and the preservation of the integrity of our profession demands nothing less.
-Wes
Acknowledgement
I am indebted to Charles P. Kroll, CPA for his invaluable assistance collecting tax records of the ABIM and ABIM Foundation before 2007 and assisting in the understanding of the nuances of not-for-profit accounting methods. Mr. Kroll provided forensic accounting analysis to the Minnesota attorney general's office during the Medica-Allina scandal and testified at the Minnesota Senate hearing on the matter.
Stop Wasting Doctors' Time (and Money)
From the New York Times today:
In my opinion, there will be much more coming soon about this sordid and very sad MOC story.
-Wes
"To rely solely on memory, especially for rarer illnesses or complicated patients, would be malpractice. Which is why the huge exam that culminates each decade of recertification should be abolished. Memorizing reams of information to be regurgitated in a “secure testing center” is a waste of time and resources, and does not reflect how medicine is practiced. Most doctors agree with having some sort of process that updates and refreshes medical knowledge. But the process has become unmanageable."Unfortunately, the well-meaning physician author of this piece does not mention the additional costs and questionable ethics of the relatively recently expanded four-step Maintenance of Certification® (MOC) process that the American Board of Medical Specialties has trademarked (and the ABIM helps implement), especially as it pertains to the research being performed on working physicians without their consent. Furthermore, the recent revelations that a shadow organization of the ABIM, the ABIM Foundation, purchased a $2.3 million luxury condominium in December 2007 after the new, more onerous MOC requirements were announced in 2005 raises many more very troubling questions about the legitimacy of this program. For instance, is MOC more about improving corporate portfolios than patient outcomes?
In my opinion, there will be much more coming soon about this sordid and very sad MOC story.
-Wes
Saturday, December 13, 2014
Electronic Medical Record and the Threat of Physician Skill Fade
As I watch the business world's fascination with the electronic medical record (EMR) and all of the Big Data that it accumulates, I see more and more processes codified and treatment pathways carefully honed. Only one small thing remains until the computer can tell doctors how to behave based on the developed algorithms: to turn free text in the patient chart into easily-definable binary pushbutton selections, so now, this is being done.
The theory, of course, is for computers to understand doctor's free text and medical decision making. By making a myriad of discrete data entry choices, we are told, recommendations for care can be made based (of course) on the best "evidence-based" guidelines the world has to offer. Data can then be quantified. Physician selections, easily followed and tracked. "Quality measures" (as defined by guidelines) "simply" quantified. This is our latest "New Vision" for health care. And as our nation hurries to implement electronic health care delivery through government mandates and regulations to assure "meaningful use" of computers, the gushing assurances of improved care spews forth from many who stand to profit from the system.
Imagine: doctors won't have to think. They'll just click the buttons and be in compliance. Stay between the lines and you're quality scores will be perfect,. Your care will be impeccable in the eyes of the developer; efficient, timely, thorough.
What could go wrong? After all, the guesswork is gone. The knowledge base clearly defined. The treatment of the disease efficiently rendered. And now, everything can be perfectly quantified.
I should acknowledge that there are clearly efficiencies gained by such a tact. But there is also a downside that really hasn't been seriously considered by most: we risk developing physician skill-fade. This, in turn, introduces a new unforseen risks to our patients since practice freedom is restricted as each algorithm demands conformity rather than innovation, improvisation, and any semblance of risk taking on the patient's behalf. After all, the computer code is optimized for its creator, the health care Iron Triangle, not the patient.
I was struck by a recent article by Nicholas Carr in the Wall Street Journal entitled, "Automation Makes Us Dumb." In it, Mr. Carr describes the benefits and challenges that automation has produced and mentions the EMR:
In fact, who needs doctors at all if care is reduced to point and click? While our new breed of physicians have never known medicine without a computer, will all of their study and preparation to become clinicians at the bedside be rendered moot as these young doctors find themselves little more than data entry clerks? How will we keep them clinically skilled? Homogenized mannequins programmed to respond to regimented scenarios?
Creating disease-directed algorithms might be efficient at treating a medical problem but this does not really treat the patient. With the infinitely variable human condition, might we be fooling ourselves with a false promise of unwavering algorithmic simplicity? Since patients rarely have one health problem but many, do these simplified treatment pathways consider the effects of other confounding ailments? Do our programmers and engineers care?
This myopic vision for medicine is where we are currently heading. Scores of centrally-created computer mandates continue to restrict the freedom of developers to move where computer-aided treatment advances need to go. As we create our linear and static algorithms that are unyielding to nuance or change (and created during a tiny snapshot of history), we should remember these limitations since physicians' freedom to act in the best interest of their patients is lost if doctors become complacent and also financially incentivized to do so. Such restriction might lower costs, but at a risk to patient care.
Realizing computers in medicine are here to stay, I can only hope that in the years ahead as computerized health records develop, a new era of computerized algorithms will evolve that adapt to any number of physician-directed exceptions and exclusions appropriately. Computers and EMRs must inform the physician rather than mandate, instruct rather than impugn, encourage adaptation rather than thwart it, and always facilitate rather than inhibit patient care. This way physician skill-fade will be minimized and a more efficient care delivery that is patient-centered rather than industry-centered can thrive.
-Wes
The theory, of course, is for computers to understand doctor's free text and medical decision making. By making a myriad of discrete data entry choices, we are told, recommendations for care can be made based (of course) on the best "evidence-based" guidelines the world has to offer. Data can then be quantified. Physician selections, easily followed and tracked. "Quality measures" (as defined by guidelines) "simply" quantified. This is our latest "New Vision" for health care. And as our nation hurries to implement electronic health care delivery through government mandates and regulations to assure "meaningful use" of computers, the gushing assurances of improved care spews forth from many who stand to profit from the system.
Imagine: doctors won't have to think. They'll just click the buttons and be in compliance. Stay between the lines and you're quality scores will be perfect,. Your care will be impeccable in the eyes of the developer; efficient, timely, thorough.
What could go wrong? After all, the guesswork is gone. The knowledge base clearly defined. The treatment of the disease efficiently rendered. And now, everything can be perfectly quantified.
I should acknowledge that there are clearly efficiencies gained by such a tact. But there is also a downside that really hasn't been seriously considered by most: we risk developing physician skill-fade. This, in turn, introduces a new unforseen risks to our patients since practice freedom is restricted as each algorithm demands conformity rather than innovation, improvisation, and any semblance of risk taking on the patient's behalf. After all, the computer code is optimized for its creator, the health care Iron Triangle, not the patient.
I was struck by a recent article by Nicholas Carr in the Wall Street Journal entitled, "Automation Makes Us Dumb." In it, Mr. Carr describes the benefits and challenges that automation has produced and mentions the EMR:
In a study conducted in 2007-08 in upstate New York, SUNY Albany professor Timothy Hoff interviewed more than 75 primary-care physicians who had adopted computerized systems. The doctors felt that the software was impoverishing their understanding of patients, diminishing their “ability to make informed decisions around diagnosis and treatment.”But what is the real issue? While the development of treatment rubrics can improve health care efficiency and productivity for their creators, I fear rote implementation of these algorithms will also also atrophy a physician's clinical and reasoning skills. Binary decisions buttons might facilitate note creation and data gathering, but they discourage the use of physical examination (remember that?) and the evaluation of nuance or clinical exceptions. With creation of our current iteration of care pathways and guidelines, there is now little need for exceptional thinkers, only adequate thinkers. What would skill fade look like in medicine? And at what point do the exceptional experienced physicians start becoming vulnerable to skill fade?
Harvard Medical School professor Beth Lown, in a 2012 journal article written with her student Dayron Rodriquez, warned that when doctors become “screen-driven,” following a computer’s prompts rather than “the patient’s narrative thread,” their thinking can become constricted. In the worst cases, they may miss important diagnostic signals.
The risk isn’t just theoretical. In a recent paper published in the journal Diagnosis, three medical researchers—including Hardeep Singh, director of the health policy, quality and informatics program at the Veterans Administration Medical Center in Houston—examined the misdiagnosis of Thomas Eric Duncan, the first person to die of Ebola in the U.S., at Texas Health Presbyterian Hospital Dallas. They argue that the digital templates used by the hospital’s clinicians to record patient information probably helped to induce a kind of tunnel vision. “These highly constrained tools,” the researchers write, “are optimized for data capture but at the expense of sacrificing their utility for appropriate triage and diagnosis, leading users to miss the forest for the trees.” Medical software, they write, is no “replacement for basic history-taking, examination skills, and critical thinking.”
In fact, who needs doctors at all if care is reduced to point and click? While our new breed of physicians have never known medicine without a computer, will all of their study and preparation to become clinicians at the bedside be rendered moot as these young doctors find themselves little more than data entry clerks? How will we keep them clinically skilled? Homogenized mannequins programmed to respond to regimented scenarios?
Creating disease-directed algorithms might be efficient at treating a medical problem but this does not really treat the patient. With the infinitely variable human condition, might we be fooling ourselves with a false promise of unwavering algorithmic simplicity? Since patients rarely have one health problem but many, do these simplified treatment pathways consider the effects of other confounding ailments? Do our programmers and engineers care?
This myopic vision for medicine is where we are currently heading. Scores of centrally-created computer mandates continue to restrict the freedom of developers to move where computer-aided treatment advances need to go. As we create our linear and static algorithms that are unyielding to nuance or change (and created during a tiny snapshot of history), we should remember these limitations since physicians' freedom to act in the best interest of their patients is lost if doctors become complacent and also financially incentivized to do so. Such restriction might lower costs, but at a risk to patient care.
Realizing computers in medicine are here to stay, I can only hope that in the years ahead as computerized health records develop, a new era of computerized algorithms will evolve that adapt to any number of physician-directed exceptions and exclusions appropriately. Computers and EMRs must inform the physician rather than mandate, instruct rather than impugn, encourage adaptation rather than thwart it, and always facilitate rather than inhibit patient care. This way physician skill-fade will be minimized and a more efficient care delivery that is patient-centered rather than industry-centered can thrive.
-Wes
Thursday, December 04, 2014
Vignettes From A Brief Foray Into Knee Surgery
The phone rang one evening and a pleasant voice was on the other end. "Hi, my name is nurse So-and-so and I'm the educational coordinator for your upcoming knee surgery. Do you want to go to the patient orientation session?" she asked. "It's very helpful to go over things before and after your surgery and to answer any questions you might have."
I thought about this. The 11am session was right smack dab in the middle of my clinical day. But I thought it best to attend and agreed.
It is not easy deciding to have an elective surgery, especially one that will sideline you from your vocation for an extended period. Some said I waited too long. Others said you should wait as long as possible. For me: two good years of limping, looking at long halls that kept getting longer and seeing my formerly active social life dwindle spurred me to proceed. It was time to surrender myself to The System.
Unfortunately, clinical demands caused me to arrive 20 minutes late to my pre-op orientation. I entered a room filled with people and their spouses, all arranged in a large semicircle facing a middle-aged nurse educator in the middle of the room. Men and women of all ages - some younger, some older. Some with partners, some without. Teams. Total knee, partial knees, hips galore!
I had no idea.
"Here's and information packet," she said as she handed me an envelope as I became one of the crowd. "I'll review what your missed at the end of the session." I took a seat as discretely as I could.
Surely if they can do this," I pondered, "I can do this."
***
"Take everything off, then wipe yourself down with one of these towelettes, then put this on," she said, handing me a neatly folded hospital gown. "Follow the directions printed here on this diagram: there are eight of these towelettes, four in each package, use one towelette for both arms, one for your chest, one for your back, one for your abdomen, then one for each leg, one for your privates, one for your butt, your wife can help you with your back…"
Welcome to being a patient!
She left and I removed my clothes. Standing buck naked in a cubicle as I changed, quite a "patient-appreciation day." It was clear this was carefully choreographed preparatory dance, held solo by a doctor who stood naked and a bit confused about the intricacies of sterile towelette application to various body parts, then wiping this part and that - especially since she forgot to tell me that the warmed towelettes cooled quickly and their evaporative loss helped redefine the term "shrinkage" as my chemical pre-operative shower concluded.. Then came the comical assembly of the hospital gown he'd seen his patients endure so many times before. In a word: dashing!
***
"Hello, doctor."
I looked up to see an man somewhat older than me, who spoke with an accent - maybe he was from India? - I wasn't sure.
"I am here to shave your leg."
"She's all yours," I said.
And with that a pair of electric shears appeared and he went to work. It was clear he enjoyed his work. "Soon you will look like Miley Cyrus," he said softly, smiling quietly to himself . Looking down at my leg a short while later, I saw a sheen on my legs that I had never seen before - damn thing looked as smooth as a baby's butt. He proudly applied adhesive tape over the area to remove the excess hair. He walked away briefly to throw the tape away and then returned. He leaned over to my wife whispering loudly enough so I could hear: "I'm so sorry," he said shaling his head, "I made a mistake."
My wife, somewhat puzzled, looked briefly concerned.
He grinned: "He looks more like Madonna."
***
"Okay, I discussed the anesthesia plan with your doctor and he and I think the best option for you would be to have a spinal for this procedure, then we'll give you some propofol and you should do fine. First, I'm going to inject you leg above your knee to give you some ongoing pain relief after your surgery. I'm going to use an ultrasound machine to infuse this area, okay?"
"Uh, sure. Less pain, more gain for me!"
I watched as he localized the vascular bundle in my adductor canal using ultrasound, then injected local. It stung just a tiny bit as he local was infused, but wasn't too severe. Piece of cake, I thought.
"Now, I'd like you to sit at the edge of the bed."
I sat dutifully at the edge of the bed, placing my head in this contraption that contained a headrest and was clearly designed for this moment - complete with foot rests and the places to place your hands. As I leaned forward, I could feel him preparing the area on my lower back, draping it with a sterile drape, then feeling for the iliac crests bilaterally. Once, then again. Then…
"You might feel a little electric shock sensation down your leg - let me know…"
And almost instantly, I felt the slightest of electric shock sensations shoot down my left leg. I brought this to his attention. He did something to relieve the mild sensation.
"There, is that better?"
"Yes," I replied, comfortable as ever.
Moments later I could feel both my legs feel warm almost instantly. They helped be lie back in bed. Within seconds, the strangest sensation occurred: paralysis. No matter how hard my brain asked my legs to move, they refused. I felt just below my belly button. Nothing to feel there, either! Paralysis, particularly while you are conscious, is a bizarre sensation. Try as you might you try to move your legs: nothing. Like a Vulcan mind meld that goes bad you try to tell you legs to do anything and… nothing. I was able to feel a tiny piece of my right 2nd toe for a bit - at least I thought I could, but nothing else. I felt oddly peaceful despite it all - probably Versed, I thought.
"We're ready to take him to the OR," they told her as the transporter and anesthesiologist assisted. "Give him a kiss."
I remembered my wife's kiss, and later moving to the OR table, and from the corner of my eye a scrub nurse in an isolation suit that looked like an Ebola isolation outfit. "Can we get him to sleep now?" I heard someone say. "Let me get his systolic above 75 first," another female voice said. "Oh great," I remembered thinking, but somehow didn't care. Clearly it was a team effort. A guy was working on my foley, but I wasn't sure - couldn't feel a thing. Somehow that part scared me the most and it was nothing. Then...
I woke bit later - minutes it seemed. To the right of me was a lady - was it a nurse? - in a lit football helmet-like head gear. What the …? The drape over her face had been removed. Others were similarly garbed: modified Ebola outfits. Cool. I want these in my OR, I thought. Drugs are an amazing thing.
"We're going to move you off the table now, Wes." And they lifted me over to a gurney. I wheeled back to the holding area, feeling victorious. The procedure I had wanted, but dreaded, was over. Now the recovery.
"You can eat when you get upstairs."
I really wasn't that hungry.
***
"Welcome to your new room. I think it's the biggest on the floor!" she exclaimed. I'm here to give you your meds. Can I have your name and date of birth?"
She clicked this and that, then gave be the pills in a small plastic cup - all kinds of them!
"The pain team has a specific regimen of medications they want you on," she explained. Not wanting to rock the boat, especially when it came to pain, I complied. If you need anything, let us know. We'll keep the ICE machine full. Let us know if you think you need more ice. Here's you incentive spirometer - 3200 cc's every hour, okay?
It was a new room, equipped with all the amenities. Classy, welcome, bigger than I needed, but I was sure it would impress the family. I could hear the saline infusion cranking quietly in the background all night. I remembered my days on the ortho ward as an intern and promised to myself: "I'll be damned if I get in-land salt water drowning! Watch the fluids."
A continuous parade of individuals from the hospital, the nurses, the technicians, PT, OT paraded through. "We try to check on you once an hour," I heard them say. I wondered when I'd get sleep. A bit after midnight it finally happened, and with another Norco sleep came easily.
***
05:50AM: "Good morning, I'm hear to draw your blood."
Heck of a wake-up call. She was young, skilled, soft-spoken. She found my vein in an instant. I learned she left home at every day at 5am, made her rounds drawing blood, then went to school.
She came early every morning, then went on her way. It was easier once we knew each other and knew what to expect each day: a confident harpooning.
***
Being a patient is a good exercise for a doctor. You an see what works, and what doesn't. You can appreciate your vulnerability and the vulnerability of your patients. I saw the coldness of the EMR and the distant computer stares as they never looked up, clicking: "Name and date of birth, please." "Tell me your name and date of birth." The another time: "Name?" "Date of birth?"
Like someone taking a mini-mental status exam on a robot.
But I also saw a team of people who were genuinely concerned with my well-being, many of whom were the people you never hear about: the orderlies, the cleaning personnel, the medical assistants, the pharmacists, and food service personnel. Not to say that the nursing, physical therapy and physician staff weren't great (they were), but it was great to see so many people not just doing their jobs, but enjoying them too.
Perhaps more than this, though, there was a humbling revelation: that like our patients, we are aging. The unlimited days of racing to a code or standing in the cath lab correcting an arrhythmia for hours at a time aren't unlimited after all. As a doctor, we've known this intellectually. But as a patient, we see this and come to appreciate this reality first-hand. And as a result, I suppose I've found a new appreciation: an appreciation for what we do and the the brevity of the time we have to do it as a doctor, the wonder of caring for patients, teaching students, and having family and loved ones that have shared this journey with us. Perhaps most of all, becoming a patient gives us a new appreciation for the finite time we have doing what we love here on this earth.
-Wes
I thought about this. The 11am session was right smack dab in the middle of my clinical day. But I thought it best to attend and agreed.
It is not easy deciding to have an elective surgery, especially one that will sideline you from your vocation for an extended period. Some said I waited too long. Others said you should wait as long as possible. For me: two good years of limping, looking at long halls that kept getting longer and seeing my formerly active social life dwindle spurred me to proceed. It was time to surrender myself to The System.
Unfortunately, clinical demands caused me to arrive 20 minutes late to my pre-op orientation. I entered a room filled with people and their spouses, all arranged in a large semicircle facing a middle-aged nurse educator in the middle of the room. Men and women of all ages - some younger, some older. Some with partners, some without. Teams. Total knee, partial knees, hips galore!
I had no idea.
"Here's and information packet," she said as she handed me an envelope as I became one of the crowd. "I'll review what your missed at the end of the session." I took a seat as discretely as I could.
Surely if they can do this," I pondered, "I can do this."
***
"Take everything off, then wipe yourself down with one of these towelettes, then put this on," she said, handing me a neatly folded hospital gown. "Follow the directions printed here on this diagram: there are eight of these towelettes, four in each package, use one towelette for both arms, one for your chest, one for your back, one for your abdomen, then one for each leg, one for your privates, one for your butt, your wife can help you with your back…"
Welcome to being a patient!
She left and I removed my clothes. Standing buck naked in a cubicle as I changed, quite a "patient-appreciation day." It was clear this was carefully choreographed preparatory dance, held solo by a doctor who stood naked and a bit confused about the intricacies of sterile towelette application to various body parts, then wiping this part and that - especially since she forgot to tell me that the warmed towelettes cooled quickly and their evaporative loss helped redefine the term "shrinkage" as my chemical pre-operative shower concluded.. Then came the comical assembly of the hospital gown he'd seen his patients endure so many times before. In a word: dashing!
***
"Hello, doctor."
I looked up to see an man somewhat older than me, who spoke with an accent - maybe he was from India? - I wasn't sure.
"I am here to shave your leg."
"She's all yours," I said.
And with that a pair of electric shears appeared and he went to work. It was clear he enjoyed his work. "Soon you will look like Miley Cyrus," he said softly, smiling quietly to himself . Looking down at my leg a short while later, I saw a sheen on my legs that I had never seen before - damn thing looked as smooth as a baby's butt. He proudly applied adhesive tape over the area to remove the excess hair. He walked away briefly to throw the tape away and then returned. He leaned over to my wife whispering loudly enough so I could hear: "I'm so sorry," he said shaling his head, "I made a mistake."
My wife, somewhat puzzled, looked briefly concerned.
He grinned: "He looks more like Madonna."
***
"Okay, I discussed the anesthesia plan with your doctor and he and I think the best option for you would be to have a spinal for this procedure, then we'll give you some propofol and you should do fine. First, I'm going to inject you leg above your knee to give you some ongoing pain relief after your surgery. I'm going to use an ultrasound machine to infuse this area, okay?"
"Uh, sure. Less pain, more gain for me!"
I watched as he localized the vascular bundle in my adductor canal using ultrasound, then injected local. It stung just a tiny bit as he local was infused, but wasn't too severe. Piece of cake, I thought.
"Now, I'd like you to sit at the edge of the bed."
I sat dutifully at the edge of the bed, placing my head in this contraption that contained a headrest and was clearly designed for this moment - complete with foot rests and the places to place your hands. As I leaned forward, I could feel him preparing the area on my lower back, draping it with a sterile drape, then feeling for the iliac crests bilaterally. Once, then again. Then…
"You might feel a little electric shock sensation down your leg - let me know…"
And almost instantly, I felt the slightest of electric shock sensations shoot down my left leg. I brought this to his attention. He did something to relieve the mild sensation.
"There, is that better?"
"Yes," I replied, comfortable as ever.
Moments later I could feel both my legs feel warm almost instantly. They helped be lie back in bed. Within seconds, the strangest sensation occurred: paralysis. No matter how hard my brain asked my legs to move, they refused. I felt just below my belly button. Nothing to feel there, either! Paralysis, particularly while you are conscious, is a bizarre sensation. Try as you might you try to move your legs: nothing. Like a Vulcan mind meld that goes bad you try to tell you legs to do anything and… nothing. I was able to feel a tiny piece of my right 2nd toe for a bit - at least I thought I could, but nothing else. I felt oddly peaceful despite it all - probably Versed, I thought.
"We're ready to take him to the OR," they told her as the transporter and anesthesiologist assisted. "Give him a kiss."
I remembered my wife's kiss, and later moving to the OR table, and from the corner of my eye a scrub nurse in an isolation suit that looked like an Ebola isolation outfit. "Can we get him to sleep now?" I heard someone say. "Let me get his systolic above 75 first," another female voice said. "Oh great," I remembered thinking, but somehow didn't care. Clearly it was a team effort. A guy was working on my foley, but I wasn't sure - couldn't feel a thing. Somehow that part scared me the most and it was nothing. Then...
I woke bit later - minutes it seemed. To the right of me was a lady - was it a nurse? - in a lit football helmet-like head gear. What the …? The drape over her face had been removed. Others were similarly garbed: modified Ebola outfits. Cool. I want these in my OR, I thought. Drugs are an amazing thing.
"We're going to move you off the table now, Wes." And they lifted me over to a gurney. I wheeled back to the holding area, feeling victorious. The procedure I had wanted, but dreaded, was over. Now the recovery.
"You can eat when you get upstairs."
I really wasn't that hungry.
***
"Welcome to your new room. I think it's the biggest on the floor!" she exclaimed. I'm here to give you your meds. Can I have your name and date of birth?"
She clicked this and that, then gave be the pills in a small plastic cup - all kinds of them!
"The pain team has a specific regimen of medications they want you on," she explained. Not wanting to rock the boat, especially when it came to pain, I complied. If you need anything, let us know. We'll keep the ICE machine full. Let us know if you think you need more ice. Here's you incentive spirometer - 3200 cc's every hour, okay?
It was a new room, equipped with all the amenities. Classy, welcome, bigger than I needed, but I was sure it would impress the family. I could hear the saline infusion cranking quietly in the background all night. I remembered my days on the ortho ward as an intern and promised to myself: "I'll be damned if I get in-land salt water drowning! Watch the fluids."
A continuous parade of individuals from the hospital, the nurses, the technicians, PT, OT paraded through. "We try to check on you once an hour," I heard them say. I wondered when I'd get sleep. A bit after midnight it finally happened, and with another Norco sleep came easily.
***
05:50AM: "Good morning, I'm hear to draw your blood."
Heck of a wake-up call. She was young, skilled, soft-spoken. She found my vein in an instant. I learned she left home at every day at 5am, made her rounds drawing blood, then went to school.
She came early every morning, then went on her way. It was easier once we knew each other and knew what to expect each day: a confident harpooning.
***
Being a patient is a good exercise for a doctor. You an see what works, and what doesn't. You can appreciate your vulnerability and the vulnerability of your patients. I saw the coldness of the EMR and the distant computer stares as they never looked up, clicking: "Name and date of birth, please." "Tell me your name and date of birth." The another time: "Name?" "Date of birth?"
Like someone taking a mini-mental status exam on a robot.
But I also saw a team of people who were genuinely concerned with my well-being, many of whom were the people you never hear about: the orderlies, the cleaning personnel, the medical assistants, the pharmacists, and food service personnel. Not to say that the nursing, physical therapy and physician staff weren't great (they were), but it was great to see so many people not just doing their jobs, but enjoying them too.
Perhaps more than this, though, there was a humbling revelation: that like our patients, we are aging. The unlimited days of racing to a code or standing in the cath lab correcting an arrhythmia for hours at a time aren't unlimited after all. As a doctor, we've known this intellectually. But as a patient, we see this and come to appreciate this reality first-hand. And as a result, I suppose I've found a new appreciation: an appreciation for what we do and the the brevity of the time we have to do it as a doctor, the wonder of caring for patients, teaching students, and having family and loved ones that have shared this journey with us. Perhaps most of all, becoming a patient gives us a new appreciation for the finite time we have doing what we love here on this earth.
-Wes
Subscribe to:
Posts (Atom)