Will CT Scan's be the next great thing to "rule out" a heart attack in the ER? It seems some think so.
In a pre-publication article from Circulation, researchers from the Massachusetts General Hospital tested the sensitivity and specificity of multi-detector CT scanning (MDCT) for the presence of calcium in the coronary arteries (or narrowing) as a surrogate for the presence of heart disease and found excellent sensitivity (100%) and fair specificity (42-82%) at predicting if a patient had an acute coronary syndrome (ACS). While the results seem promising, there were important limitations to the application of this technology to a large ER population. Of 306 patients, only 123 were eligible to consent. Why? Because the study excluded people with heart rhythm abnormalities (this effects the quality of the CT scans obtained), their kidney function was too abnormal (creatinine > 1.3) or they were allergic to iodine (renotoxic iodine contrast is used for this study. Others reasons cited for not performing the scans was because some patients ruled in for heart problems with more conventional tests or they were immediately discharged.
Nonetheless, of those with an uncertain diagnosis, CT scanning with MDCT has a strong negative predictive power of 100% (that is, if patients did not have evidence of plaque or stenosis on CT scanning, they were not likely to have disease), but a positive predictive value of 23% (presence of plaque did not mean the person had an acute coronary event very well.) In appropriately selected patients, this should add to our ability to avoid admission in a larger subset of patients presenting with weird chest discomfort in the Emergency Room.
The (multi-)million dollar question is this: who will pay for this scanning? Sure the patient with an uncertain chest pain diagnosis might be able to find out their fate more quickly, but broad scale use of these scans will be VERY expensive for our health care system.
There is significant pressure by government agencies to limit CT scan imaging in ER's. And as we've seen, if these scans aren't reimbursed, few people are likely to receive them.
-Wes
Tuesday, October 31, 2006
Halloween Grand Rounds
WIth a spin on "The Raven" by Edgar Allen Poe, Dr. Hebert's Medical Gumbo presents, "The Intern":
-Wes
Once upon a midnight dreary, while I rounded weak and wearyHappy Halloween!
Stomach hot and rumbling, I came bleary and a-stumbling
For a cup of hot caffeine through the doctor’s parlor door.
On the sofa lurked before me a shadow breaking silence with rumbling snore.
‘Tis some visitor, I muttered, slumb’ring loudly, bell'wing out that roar.
A sleeping Intern, nothing more.
...
-Wes
Monday, October 30, 2006
Energy Drinks: Rocket Fuel for the Heart

Red Bull. Monster. Rockstar. All rocket fuel for the heart. But the kids are drinking it up like never before. Wonder why your child notes their heart skip or race? Ask about how many of these drinks they have a day. You'll be amazed.
It turns out that my son likes this stuff. I tried one this weekend for the first time. I did the "sugar free" variety." It was bad, but then, I know this stuff wasn't marketed to folks who can consume other "stimulating" beverages. No, this is for kids.
What I've been impressed with is how Red Bull took over my son's high school: a young man came up to their Red Bull car and was recruited. How? Free Red Bull for all the years he's in high school provided he gave it away to all of his friends. He's one of the most popular kids in his school. Gorilla marketing at its most powerful.
But this stuff can make you sick. Too much of this stuff can definitely cause symptoms: skipped heart beats, racing heart, anxiety, nervousness, hyperventillation with its associated numbness in the hands and feet, and in kids with underlying heart disorders, it can certainly exacerbate preexisting heart rhythms. Our pressured kids are drinking this stuff to stay awake long enough to do their homework after gaming too late at night or staying up on their cell phones talking to their girlfriends or boyfriends ("Who needs sleep?" I've heard kids say.)
But the biggest worry is how some teens use the drinks. Some report downing several cans in a row to get a buzz, and a new study found a surprising number of poison-center calls from young people getting sick from too much caffeine.Starting to sound a bit like the cigarette industry, doesn't it?
Danger only adds to the appeal, said Bryan Greenberg, a marketing consultant and an assistant professor of marketing at Elizabethtown College.
And don't get me started on how ridiculously expensive these drinks are...
I guess you have to pay for all those freebies somehow.
-Wes
Sunday, October 29, 2006
Purell and the Power of Marketing

In 1997, Purell was introduced to the marketplace and has swept the world with its claims of removing "99.9% of bacteria" from surfaces. Even politicians, it seems,are now getting into the act, using a spritz of the goo to clean their hands after shaking the hands of their constituents.
But what are the data here? You know, the REAL data. Is this goo as good as it's advertized? I decided to spend a minute looking for some data and review of what others have found. It's pretty interesting.
Take for instance, that most of the "99.9% bacterial free" studies were done on inanimate surfaces, not human hands. In fact, in one study, the number of bacterial colonies on neonatal nurses' hands after using the stuff was found to be "3.11 x log10" and was no different (statistically) than plain hand washing ("3.21 x log10"). Whoa there. Let's write out the numbers of bacteria on those alcohol gel hands:
31,100,000,000 colonies of bacteria were STILL THERE after the use of alcohol-based goo! Hardly sterile. No wonder I never use this stuff before surgery. But obsessive compulsives can rejoice! No need to rid yourself of your hand-washing compulsion, there's still tons of bacteria left over that NEED your attention!
And even the FDA has questioned the claims of "antibacterial" products as well:
In the documents released yesterday, the FDA said it found no medical studies that showed a link between a specific consumer antibacterial product and a decline in infection rates. Indeed, one major study found little difference between washing with soap and using an antimicrobial product. However, the agency said that the data about links to resistant strains of bacteria are "conflicting and unclear." The worries raised by researchers center largely on triclosan, an ingredient in a number of antibacterial products.But Purell and its congeners are less irritating to our skin compared to repetitive handwashing, so health care providers might be more apt to use it. Fair enough.
The issues of what we're doing to our immune systems is now coming into question, especially with the high prevalence of asthma in kids these days. We have known about "super bugs" like methicillin-resistant staph. aureus, or c. difficile. One wonders if we're selecting out these critters using antimicrobial products and alcohol-based gels. This piece from Salon.com does a nice job on presenting the drawbacks that might be inherent to using all these products.
Some bacteria are good for us. They are part of what makes us tick. Take, for instance, folks taking the blood thinner, warfarin (Coumadin(R)). Warfarin blocks the production of Vitamin K which is integral to allowing our blood to clot. Vitamin K has several sources: some is produced in the liver, some exists in our diet, and some is produced by bacteria in our gut. Antibiotics administered to people on warfarin can kill many of the gut bacteria that make Vitamin K, causing the person's blood to become "too thin" if the dose of warfarin is not adjusted accordingly. So in this case, bacteria can be helpful to us, provided we do not disturb nature's careful homeostasis.
Maybe these politicians using this stuff should clean up their acts before cleaning their hands. Our health care system would be a great place to start.
-Wes
Saturday, October 28, 2006
Influenza Vaccine - Worthless?
A critical review of the data regarding the effectiveness of the influenza vaccine from the British Medical Journal:
-Wes
The optimistic and confident tone of some predictions of viral circulation and of the impact of inactivated vaccines, which are at odds with the evidence, is striking. The reasons are probably complex and may involve "a messy blend of truth conflicts and conflicts of interest making it difficult to separate factual disputes from value disputes" or a manifestation of optimism bias (an unwarranted belief in the efficacy of interventions).Interesting read and worth a look. I think the difficulty clinically is the lack of a rapid, reliable test to confirm the diagnosis of influenza.
-Wes
Friday, October 27, 2006

The New Big Blue Box
Well, just when I thought I had nothing to blog about, I was given a gift. Today’s topic: plastics.
I had my first opportunity to use Medtronic’s Adapta and Versa pacemakers today. Nice line, but no big paradigm shift from last year’s models. What WAS different, however, was the packaging: each of these pacemakers were packaged in a fairly thick Big Blue plastic box emblazoned with a beautiful Medtronic logo. Not cardboard, as in prior years’ models. Nope, non-biodegradable, last-for-ever, oil-cartel supporting, plastic. I guess trees in ol’ Minnesota are getting thin, so they went with plastic. Or could there be another reason… Hmmmm…

Remember that meeting between Art Collins and Carlos Gutierrez earlier this year? Could this have been what the Bush administration wanted: the use of plastic to support big oil interests? Maybe it’s cheaper to manufacture, I really don’t know. But like it or not, the long-term implications of packaging like this are significant. Other big corporations like McDonalds got rid of their Styrofoam clam-shell packaging for their Big Macs in favor of cardboard boxes due to grass-roots pressure. Even Starbucks has been pressured to bring back paper cups in many of its stores. Now I don’t consider myself particularly “Green,” but with the price of oil these days, it seems it should be cheaper to package in cardboard rather than plastic – certainly it seems better for our environment.
And how do hospitals get rid of their trash? All this trash was commonly incinerated and this has been a sensitive topic here in Illinois. Landfills are no better, since this stuff will never decompose.
Now don’t get me wrong. Medtronic is a fine company and makes great products. But decisions to make packaging changes should be examined carefully, especially when they have such an important world-wide impact for our patients and environment.
-Wes
I had my first opportunity to use Medtronic’s Adapta and Versa pacemakers today. Nice line, but no big paradigm shift from last year’s models. What WAS different, however, was the packaging: each of these pacemakers were packaged in a fairly thick Big Blue plastic box emblazoned with a beautiful Medtronic logo. Not cardboard, as in prior years’ models. Nope, non-biodegradable, last-for-ever, oil-cartel supporting, plastic. I guess trees in ol’ Minnesota are getting thin, so they went with plastic. Or could there be another reason… Hmmmm…

Remember that meeting between Art Collins and Carlos Gutierrez earlier this year? Could this have been what the Bush administration wanted: the use of plastic to support big oil interests? Maybe it’s cheaper to manufacture, I really don’t know. But like it or not, the long-term implications of packaging like this are significant. Other big corporations like McDonalds got rid of their Styrofoam clam-shell packaging for their Big Macs in favor of cardboard boxes due to grass-roots pressure. Even Starbucks has been pressured to bring back paper cups in many of its stores. Now I don’t consider myself particularly “Green,” but with the price of oil these days, it seems it should be cheaper to package in cardboard rather than plastic – certainly it seems better for our environment.
And how do hospitals get rid of their trash? All this trash was commonly incinerated and this has been a sensitive topic here in Illinois. Landfills are no better, since this stuff will never decompose.
Now don’t get me wrong. Medtronic is a fine company and makes great products. But decisions to make packaging changes should be examined carefully, especially when they have such an important world-wide impact for our patients and environment.
-Wes
Suffering Blogopenia
Blogopenia – Definition: adj. suffering from writer’s block, lack of material on which to blog
Etymology: blog: 1999-2004; abbreviation of Weblog and -penia: (New Latin from the Greek: peni): lack, deficiency.
I starting writing my blog this morning and noticed that the word “Blog” was underlined by my spell-checker on my Mac software, Word 2004. Newer spell-checkers now ignore the term and Dictionary.com has it on their website, so the word “blog” is now firmly added to our vernacular.
In my perusing of other blogs, I noticed some other medical suffixes applied to the word “blog,” like blogorrhea (people who blog too much or expound beyond reasonable limits). I just thought I’d add this word to my blogging vernacular this AM since I’m definitely “blogopenic.”
Maybe there are other terms out there and we could start our own blogging dictionary!
-Wes
08:25 AM C.S.T.: Addendum: From Musemonkey: As always, seems I'm a day late to this party.
Etymology: blog: 1999-2004; abbreviation of Weblog and -penia: (New Latin from the Greek: peni): lack, deficiency.
I starting writing my blog this morning and noticed that the word “Blog” was underlined by my spell-checker on my Mac software, Word 2004. Newer spell-checkers now ignore the term and Dictionary.com has it on their website, so the word “blog” is now firmly added to our vernacular.
In my perusing of other blogs, I noticed some other medical suffixes applied to the word “blog,” like blogorrhea (people who blog too much or expound beyond reasonable limits). I just thought I’d add this word to my blogging vernacular this AM since I’m definitely “blogopenic.”
Maybe there are other terms out there and we could start our own blogging dictionary!
-Wes
08:25 AM C.S.T.: Addendum: From Musemonkey: As always, seems I'm a day late to this party.
Thursday, October 26, 2006
Carotid Stent Debate - Dissin' the French

Today's New York Times discussed the carotid stenting debate going on over at the TCT. Seems doctors are dissin' the French study from the New England Journal of Medicine last week demonstrating superiority of surgical endarterectomy over carotid stenting.
“No one wants a scar on their neck when they can have a Band-Aid on their groin,” said L. Nelson Hopkins, a professor of neurosurgery and radiology at the State University at Buffalo School of Medicine. ...But a closer look at the French study demonstrates the issue of distal protection devices (little umbrellas that catch debris as seen in Panel B (small arrow) above) was reviewed, and it was decided to stop the study anyway:
The more worrisome report was published last week in the New England Journal of Medicine, which told of a trial in France halted even before it finished enrolling patients after data on the first 527 showed that 9.6 percent of them had died or suffered strokes within 30 days compared to just 3.9 percent of those who underwent surgery.
Doctors here said that both studies had numerous shortcomings that made the results unreliable. The drawbacks, they said, included failure in many of the stenting cases for physicians to use a protective filter that is required in all American procedures and is designed to catch bits of life-threatening plaque knocked loose during the procedure.
The relative risk of stroke or death did not differ significantly among the centers that enrolled fewer than 21 patients (relative risk, 1.9; 95% CI, 0.6 to 6.2), those that enrolled 21 to 40 patients (relative risk, 3.3; 95% CI, 0.7 to 15.2), and those that enrolled more than 40 patients (relative risk, 2.7; 95% CI, 0.9 to 8.1) (P=0.83). The 30-day incidence of stroke or death was similar among patients treated by interventional physicians who were experienced (11 of 105, or 10.5%), tutored during training (7 of 98, or 7.1%), and tutored after training (7 of 57, or 12.3%) (P=0.54; chi-square statistic, 1.25).Where it might be nicer to have a bandaid on your groin than a scar on your neck, if the risk of stroke is indeed higher with carotid stenting, then I'd rather be able to walk with a scar on my neck, than be paralyzed with a bandaid on my groin.
The 30-day incidence of stroke or death was lower among patients who underwent stenting with cerebral protection (18 of 227, or 7.9%) than among those treated with stenting alone (5 of 20, or 25%; P=0.03). However, the relative risk of stroke or death for stenting over endarterectomy did not differ significantly before systematic use of a cerebral protection device was recommended (2.0; 95% CI, 0.8 to 5.0) or after (3.4; 95% CI, 1.1 to 10.0; P=0.50).
We'd better go slowly here and make sure marketing pressures don't cloud our judgement - even IF the stenting market is likely to be a $1 billion market, as the article suggests.
-Wes
Photo credit.
Wednesday, October 25, 2006
The Health Care Flush
This morning’s Wall Street Journal (subscription required) discloses another problem with health care costs: pharmaceutical special interests on Capital Hill. It seems the drug companies are pumping millions into campaigns for our elected fearless leaders in an interest to sway the vote. Here’s an outline of the Top 10 contributions:
Rick Santorum (R, PA) - $454, 500
Orrin Hatch (R Utah) - $301, 050
Joe Lieberman (I, Conn.) - $240, 740
Mike Ferguson (R, NJ) - $239, 670
Edward Kennedy, (D, Mass.) - $226, 550
Mike DeWine (R, Ohio) - $214,040
Nathan Deal (R, Georgia) - $183, 590
Jon Kyl (R, Arizona) - $179, 500
Nancy Johnson (R, Conn) - $171, 460
Ben Nelson (D, Nebraska) - $169, 890
Total contributions, just with these ten: $2,380, 990! * Ka-ching! *
You can bet there are MANY others. * Ka – ching! *
Don’t let those imports of cheaper drugs occur! * Ka – ching! *
These 10 contributions represent 238 more people without a year’s worth of health care coverage…
* flush * goes the toilet…
-Wes
Rick Santorum (R, PA) - $454, 500
Orrin Hatch (R Utah) - $301, 050
Joe Lieberman (I, Conn.) - $240, 740
Mike Ferguson (R, NJ) - $239, 670
Edward Kennedy, (D, Mass.) - $226, 550
Mike DeWine (R, Ohio) - $214,040
Nathan Deal (R, Georgia) - $183, 590
Jon Kyl (R, Arizona) - $179, 500
Nancy Johnson (R, Conn) - $171, 460
Ben Nelson (D, Nebraska) - $169, 890
Total contributions, just with these ten: $2,380, 990! * Ka-ching! *
You can bet there are MANY others. * Ka – ching! *
Don’t let those imports of cheaper drugs occur! * Ka – ching! *
These 10 contributions represent 238 more people without a year’s worth of health care coverage…
* flush * goes the toilet…
-Wes
Bioabsorbable Stent May Have Promise
From the Chicago Tribune:
-Wes
The absorbable stent is made of polylactic acid, which is used in other medical products such as sutures used to close wounds after surgery and also absorb into the body, researchers say. It is coated with the same drug that Abbott uses on its drug-coated metal stent, known as Xience. The stent has been approved in Europe and Abbott will submit it to U.S. regulators next year for approval in 2008.But 30 patients so far (and 30 days of follow-up) in the US is still a small number.
Abbott's study so far involves just 30 patients who have had the absorbable stents implanted for just 30 days, but Abbott and researchers involved with the product said it seems to be safe and shows no sign of clotting or other harmful side effects so early in the clinical trial process.Ah, the power of marketing. I just wish companies, in their rush to have early results for big (money) meetings like the TCT meeting in Washington this week, would refrain from such press releases until longer follow-up and real safety data are available. It reveals the subterranian motives of our pharmaceutical industry: stock prices are more important than patient well-being.
-Wes
Tuesday, October 24, 2006
Swimmers and Cell Phones
My cell phone’s internet connection icon whirred as I checked my Sitemeter stats. Only my faithful Three Readers today. Damn, I thought, as my gonads shriveled further. My poor little swimmers took a hit with that check, I learned. But maybe that’s a good thing…. I’ve got three healthy kids after all!
Let’s see, check my e-mail, check Sitemeter again, check my other e-mail, check my third e-mail, check work e-mail, check Bloglines, check my voicemail. Check them again. (After all, I am a * sniff * Blogaholic!)
“Honey?”
“Yes, dear?”
“I think it’s safe now.”
“Safe for what?”
“Well, given my cellular exposure, I should be shooting blanks.”
“Get a life.”
‘nough said.
-Wes
Let’s see, check my e-mail, check Sitemeter again, check my other e-mail, check my third e-mail, check work e-mail, check Bloglines, check my voicemail. Check them again. (After all, I am a * sniff * Blogaholic!)
“Honey?”
“Yes, dear?”
“I think it’s safe now.”
“Safe for what?”
“Well, given my cellular exposure, I should be shooting blanks.”
“Get a life.”
‘nough said.
-Wes
Grand Rounds 3.5 is Up
The first medical blogging Grand Rounds to be hosted by a brave lawyer, Bob Coffield of West Virginia, is up at the Health Care Law Blog.
-Wes
-Wes
A Wonderful Life
It has been a particularly rough week. Not from work and all. Heck, work has been surprisingly light this week. It’s not really about me. No, it really isn’t. I know what it is, but I hesitate to mention it. I really don’t want to think about it. It’s even tough to blog about. But I know, deep in my heart and beyond all rationalization, that my father is dying. Damn, it’s tough to type that word! There – I said it. Tears. Damn.
He just turned 83. Shortly thereafter, he fell. Happy birthday. For the elderly, that four-letter word is the nastiest of all: F-A-L-L. Falls can happen for a myriad of reasons, none of them good when you’re his age. His internist wisely admitted him in an attempt to sort through the 19 medical problems on his problem list. And after a week in the hospital, his problem list grew to 20. But tears and counting can’t fix things, can they? After all, we’re all dying, really. Just he’s a bit closer in the journey of life, I guess. So I’d rather focus on the positive – the wonderful things that he gave to me, my mother, and siblings. What else can I do when God’s inexorable pull to return us to earth continues?
This weekend while his rump has solidly glued to the hospital bed, I joined him a bit before noon to watch football on the hospital TV. He was eating lunch when I came in. I brought some pictures my wife had assembled years ago in a photo album for me. We sat at first, watching the football game unfold. It was exciting at times, but he was struggling to lift the fork to his mouth. A large piece of rubber chicken sat in the middle of his plate, untouched. He had always loved chicken. But his arms were too weak to lift the knife and fork to cut the piece of rubber, so I helped him. I cut the hell out of that chicken to render it into tiny bite-sized chunks for easy consumption. He smiled, said “thank you,” and proceeded to devour the entire plate-full of food. Wonderful. “Food is medicine,” the doctor in me told him. “Sorry, Dad,” my heart whispered.
After a commercial break I reached for the photo album. “I brought in a few pictures.”
“Really?”
“Yeah, it’s like a ‘This is Your Life’ book Diane made for me.”
I opened to the first picture and there it was: a picture of my father holding me in his arms as a baby, with my brother and sister smiling next to him. It was grey, streaked, much like his body now.
“Oh, my God! Look at that!” And a smile came over his face. “Can you believe?” He looked at me. No, it’s hard to believe Dad. And quickly his eyes devoured the pictures just as his mouth had consumed the rubber chicken. Football was unimportant. Life mattered. His life. The TV was turned off. We turned the pages one by one, slowly, patiently, eagerly, revealing my life, certainly, but his life, too. Each picture with its own story – none of them sad. Vacations, birthday parties, Winter Dance as a teen, gymnastics victories, the birth of grandkids. Wonderful memories all. None of them painful. His knees and shoulders were forgotten, but for a moment. If only I could freeze time then. No pain, no worries, no sadness, no struggles. Just joy reflecting. It did us both good. We talked. He shared a few more of his concerns and remembrances. He spoke strong and proud. “It goes so fast, doesn’t it?”
And soon the dailies of hospital life encroached – the food service folks picked up his tray, another blood draw, recording the “I&O’s” (intake and output), and I had to hurry off to join my son to attend, what else, but a football game.
Yes, Dad, fast indeed.
-Wes
He just turned 83. Shortly thereafter, he fell. Happy birthday. For the elderly, that four-letter word is the nastiest of all: F-A-L-L. Falls can happen for a myriad of reasons, none of them good when you’re his age. His internist wisely admitted him in an attempt to sort through the 19 medical problems on his problem list. And after a week in the hospital, his problem list grew to 20. But tears and counting can’t fix things, can they? After all, we’re all dying, really. Just he’s a bit closer in the journey of life, I guess. So I’d rather focus on the positive – the wonderful things that he gave to me, my mother, and siblings. What else can I do when God’s inexorable pull to return us to earth continues?
This weekend while his rump has solidly glued to the hospital bed, I joined him a bit before noon to watch football on the hospital TV. He was eating lunch when I came in. I brought some pictures my wife had assembled years ago in a photo album for me. We sat at first, watching the football game unfold. It was exciting at times, but he was struggling to lift the fork to his mouth. A large piece of rubber chicken sat in the middle of his plate, untouched. He had always loved chicken. But his arms were too weak to lift the knife and fork to cut the piece of rubber, so I helped him. I cut the hell out of that chicken to render it into tiny bite-sized chunks for easy consumption. He smiled, said “thank you,” and proceeded to devour the entire plate-full of food. Wonderful. “Food is medicine,” the doctor in me told him. “Sorry, Dad,” my heart whispered.
After a commercial break I reached for the photo album. “I brought in a few pictures.”
“Really?”
“Yeah, it’s like a ‘This is Your Life’ book Diane made for me.”
I opened to the first picture and there it was: a picture of my father holding me in his arms as a baby, with my brother and sister smiling next to him. It was grey, streaked, much like his body now.
“Oh, my God! Look at that!” And a smile came over his face. “Can you believe?” He looked at me. No, it’s hard to believe Dad. And quickly his eyes devoured the pictures just as his mouth had consumed the rubber chicken. Football was unimportant. Life mattered. His life. The TV was turned off. We turned the pages one by one, slowly, patiently, eagerly, revealing my life, certainly, but his life, too. Each picture with its own story – none of them sad. Vacations, birthday parties, Winter Dance as a teen, gymnastics victories, the birth of grandkids. Wonderful memories all. None of them painful. His knees and shoulders were forgotten, but for a moment. If only I could freeze time then. No pain, no worries, no sadness, no struggles. Just joy reflecting. It did us both good. We talked. He shared a few more of his concerns and remembrances. He spoke strong and proud. “It goes so fast, doesn’t it?”
And soon the dailies of hospital life encroached – the food service folks picked up his tray, another blood draw, recording the “I&O’s” (intake and output), and I had to hurry off to join my son to attend, what else, but a football game.
Yes, Dad, fast indeed.
-Wes
Monday, October 23, 2006
Women Helped After Open Heart Surgery
Sometimes the simplest things are great ideas. How many times do we see patients find relief from post-operative pain by clutching heart-shaped pillows across their chests after open-heart surgery? It seems logical that this bra helps.
Only thing is... I know some pretty big guys who would have benefited from a similar device.
-Wes
Only thing is... I know some pretty big guys who would have benefited from a similar device.
-Wes
Long-Acting Carvedilol Available in 2007
From Glaxo Smith Kline's PR release:
-Wes
COREG CR will utilize Flamel's proprietary Micropump® technology, which controls the delivery of carvedilol helping to maintain appropriate amounts of medicine in the body over a 24-hour span. This technology allows COREG CR to be dosed once daily, in contrast to immediate-release COREG (carvedilol) tablets, which patients must take twice daily. GlaxoSmithKline plans to begin shipping COREG CR in the first quarter of 2007.This is an important drug for our patients with severe heart failure, based on the data from the COMET trial. The pricing is not yet available, but look for it to be a bit more than two standard Coreg tablets.
-Wes
Sunday, October 22, 2006
Infection: A Cause of Cardiac Stent Thrombosis?
If we know that sterile technique is important to reduce infection in the cardiac electrophysiology laboratory when implanting foreign bodies like pacemakers and defibrillators, why do interventional cardiologists feel the risks of implanting foreign bodies like bare-metal or drug-eluting stents are less likely to become infected?
Now let me be clear. I have no data on this subject. Certainly when fevers develop after an angioplasty we might consider stent infection in the differential diagnosis of post-stenting fever. But could subclinical infection without fever be a cause of stent thrombosis? I know that the practice of not wearing surgical masks and hats is common in many cath labs around the country. Yesterday AM in the New York Times we saw yet another cardiologist without a hat or mask while performing an interventional cardiac procedure. Note that the technician assisting the doctor is wearing the mask and hat (and protective goggles).
But take a look at this high-speed picture of the average sneeze:

What kind of critters are spread widely in the lab setting when this occurs? Speech spreads bacteria in a similar fashion.
This is a particularly perplexing problem because localized stent infection just might (and I emphasize the word "might") be a cause of in-stent thrombosis. Since in-stent thrombosis and sudden late clotting of stents has recently come to the forefront of cardiologists' conciousness, as well as the conciousness of medical device companies like Boston Scientific, Medtronic and Cordis, why are we not having this discussion? Admittedly this conjecture is extremely difficult to prove or disprove. Stents are small and fixed into critical blood vessels supplying the heart muscle. Systemic symptoms may NOT be seen because of the tiny size of the devices. (When was the last time you had a fever when a splinter was caught in your foot?) Removing a stent for "culture" is impossible once the device is deployed in the coronary artery (short of open heart surgery and bypass). But fastidious organisms that grow slowly are well-described in the infectious disease and cardiology literature.
Before we start blaming drug-eluting stents as the problem, perhaps we ought to examine our own practices more carefully. Could we be part of the recently-discovered problem with in-stent thrombosis?
Hey, this might be a cool project....
-Wes
Now let me be clear. I have no data on this subject. Certainly when fevers develop after an angioplasty we might consider stent infection in the differential diagnosis of post-stenting fever. But could subclinical infection without fever be a cause of stent thrombosis? I know that the practice of not wearing surgical masks and hats is common in many cath labs around the country. Yesterday AM in the New York Times we saw yet another cardiologist without a hat or mask while performing an interventional cardiac procedure. Note that the technician assisting the doctor is wearing the mask and hat (and protective goggles).
But take a look at this high-speed picture of the average sneeze:

What kind of critters are spread widely in the lab setting when this occurs? Speech spreads bacteria in a similar fashion.
This is a particularly perplexing problem because localized stent infection just might (and I emphasize the word "might") be a cause of in-stent thrombosis. Since in-stent thrombosis and sudden late clotting of stents has recently come to the forefront of cardiologists' conciousness, as well as the conciousness of medical device companies like Boston Scientific, Medtronic and Cordis, why are we not having this discussion? Admittedly this conjecture is extremely difficult to prove or disprove. Stents are small and fixed into critical blood vessels supplying the heart muscle. Systemic symptoms may NOT be seen because of the tiny size of the devices. (When was the last time you had a fever when a splinter was caught in your foot?) Removing a stent for "culture" is impossible once the device is deployed in the coronary artery (short of open heart surgery and bypass). But fastidious organisms that grow slowly are well-described in the infectious disease and cardiology literature.
Before we start blaming drug-eluting stents as the problem, perhaps we ought to examine our own practices more carefully. Could we be part of the recently-discovered problem with in-stent thrombosis?
Hey, this might be a cool project....
-Wes
Medical Mystery Solved
Many years ago, my wife and I were exploring rural Pennsylvania and decided to stop at a road-side antique store. I was collecting antique medical instruments at the time and asked the lady inside the store if she knew of any items relating to medicine. She didn't recall seeing any. But because the store was packed with various items of all types, we decided to look anyway.
Toward the back of the store we noted lots of luggage and handbags. I looked through them and found this:

Upon opening this bag I peered inside and much to my delight, found this:

Careful inspection disclosed surgical knives, a tourniquet, trephining burr (used for boring holes in the head to remove demons causing epilepsy, insanity, or worse) and a saw – likely used for amputation. In the corner of the kit, was this sterile catgut suture dispenser, for No. 1, No. 2, and No. 3 catgut suture, made by Johnson & Johnson, of New Brunswick, NJ, USA. (Hence the "hint" of my prior post: a "cat's gut"... my apologies to cat lovers out there ...)

The only markings on the equipment were those of the packages of sutures and bandages inside. At first I thought the kit was a post-mortum surgical kit, but the findings of the trephine and the sterile catgut (why would a mortician need sterile catgut?) made a surgical amputation kit near the turn of the 20th century more likely. Although I have not been able to identify which company made the kit, I was able to find some information on the Johnson and Johnson website that helped me date the kit. From Johnson and Johnson's website:
Despite all of our modern-day rants, it certainly reminds us that Medicine has come a long way...
-Wes
Toward the back of the store we noted lots of luggage and handbags. I looked through them and found this:

Upon opening this bag I peered inside and much to my delight, found this:

Careful inspection disclosed surgical knives, a tourniquet, trephining burr (used for boring holes in the head to remove demons causing epilepsy, insanity, or worse) and a saw – likely used for amputation. In the corner of the kit, was this sterile catgut suture dispenser, for No. 1, No. 2, and No. 3 catgut suture, made by Johnson & Johnson, of New Brunswick, NJ, USA. (Hence the "hint" of my prior post: a "cat's gut"... my apologies to cat lovers out there ...)
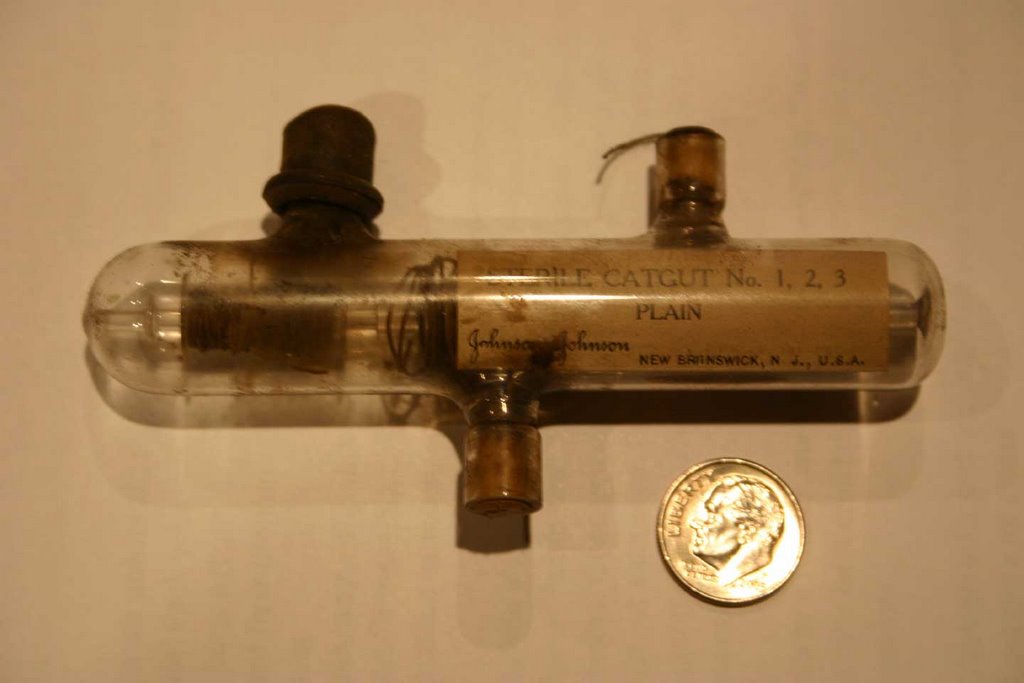
The only markings on the equipment were those of the packages of sutures and bandages inside. At first I thought the kit was a post-mortum surgical kit, but the findings of the trephine and the sterile catgut (why would a mortician need sterile catgut?) made a surgical amputation kit near the turn of the 20th century more likely. Although I have not been able to identify which company made the kit, I was able to find some information on the Johnson and Johnson website that helped me date the kit. From Johnson and Johnson's website:
By 1890 Johnson & Johnson was treating cotton and gauze dressings by dry heat in an attempt to produce not only an antiseptic product but a sterile one. In 1891 a bacteriological laboratory was established and, early in the following year, the Company successfully met the requirements for a sterile product through a continuous method of handling dressings so they were kept under aseptic conditions and subject to repeated sterilization during production.I have often wondered about the history of this kit. Was it ever used? If so, on whom? What were the circumstances of their injuries? Was anesthesia used? I imagine a solution or a spray of carbolic acid bathing the operating room and the patient in a foggy mist while the surgeon operates in street clothes with a blood-spattered frock coat worn like a badge of honor.
The new sterilization processes, first by dry heat and then by steam and pressure, were the genesis of the Company's slogan: "The Most Trusted Name in Surgical Dressings." In 1897 the Company developed another major contribution to surgery, an improved sterilizing technique for catgut sutures.
Despite all of our modern-day rants, it certainly reminds us that Medicine has come a long way...
-Wes
Saturday, October 21, 2006

Medical Mystery

Since Dr. A has had some fun posting pictures of unknowns recently, I thought I would follow his lead with this photo. What is it?
(Note I placed a dime near it as a size reference. I have a thing about dimes....)
-Wes
(Answer tomorrow...)
Friday, October 20, 2006
Playground Games
It was 11:45 AM on a clear October morning. A group of about fifty children were busy with activities like hop-scotch, throwing a football, chatting and clowning around. A large group of kids had assembled in a circle toward the corner of the black-top surface near one end of the basketball court, so I wandered over.
A dark-haired boy was encircling the seated kids, placing his hand on each seated child’s head.
“Duck, duck, duck, duck, duck, duck, GOOSE!”
And with the word “goose,” the blonde-haired girl jumped up and tried to chase the boy around the circle and tag him before he could sit down at the previously abandoned spot. She missed, so she became the “goose” and the game continued.
“Duck, duck, duck, duck, duck, duck, duck, duck, GOOSE!”
This time, a dark-haired girl with wire-rim classes rose and chased the blonde girl and tagged her. The blonde girl had to stay the goose. On and on it went.
Several minutes later I noticed a small girl with downcast eyes behind large dark glasses with quivering shoulders. I approached her.
“Sarah?”
“Uh, huh.”
“Are you, OK?”
She didn’t respond. Her shoulders quivered faster. It was clear she was crying and embarrassed to reveal herself in such a state.
“What’s wrong, Sarah?” I asked.
She paused, lip quivering. Her bright blue eyes were full of tears as she looked up at me. “I…. I… I never get GOOSED!”
Sometimes it’s good to get goosed in life. It’s important to feel included, even if there are risks in doing so. It was with amazement that I learned in an editorial from the Chicago Tribune about Willett Elementary School in Attelboro, Massachusetts banning any game incorporating tag.
Unstructured play time is incredibly important for our children as confirmed by the American Academy of Pediatrics. Furthermore, the benefits of games like “tag” increases physical activity in our children and helps reduce obesity, too. But beyond the physical benefits, teaching our children what life is about – that competition exists and is part of life – that we cannot always “win” and must learn how to cope when we lose – these are the most important lessons we learn in our formative years, are they not?
I ran today’s Tribune editorial by an expert: my daughter, age 11. “What do you think about this?” I asked her.
“Oh Daddy, that’s nothing. You think that’s bad? Guess what all of our teachers tell us when we want to play Tug-of-War?”
I had no idea.
“We can’t call it that, Daddy.”
“Why not?”
“They think it’s too mean to call it Tug-of-War – we have to call it Tug-of-Peace.”
I couldn’t believe my ears. In our neighborhood, our Great American Public school system no longer condones the term “Tug-of-War” on the playground. The ridiculousness of the re-naming was not lost on my 11-year-old daughter. It is both condescending, patronizing, and disingenuous to her. Unfortunately, it seems “war” now so politically incorrect that we can no longer use the term at our school.
A quick question for our "teachers:"
Are we at "peace" in Iraq?
-Wes
A dark-haired boy was encircling the seated kids, placing his hand on each seated child’s head.
“Duck, duck, duck, duck, duck, duck, GOOSE!”
And with the word “goose,” the blonde-haired girl jumped up and tried to chase the boy around the circle and tag him before he could sit down at the previously abandoned spot. She missed, so she became the “goose” and the game continued.
“Duck, duck, duck, duck, duck, duck, duck, duck, GOOSE!”
This time, a dark-haired girl with wire-rim classes rose and chased the blonde girl and tagged her. The blonde girl had to stay the goose. On and on it went.
Several minutes later I noticed a small girl with downcast eyes behind large dark glasses with quivering shoulders. I approached her.
“Sarah?”
“Uh, huh.”
“Are you, OK?”
She didn’t respond. Her shoulders quivered faster. It was clear she was crying and embarrassed to reveal herself in such a state.
“What’s wrong, Sarah?” I asked.
She paused, lip quivering. Her bright blue eyes were full of tears as she looked up at me. “I…. I… I never get GOOSED!”
Sometimes it’s good to get goosed in life. It’s important to feel included, even if there are risks in doing so. It was with amazement that I learned in an editorial from the Chicago Tribune about Willett Elementary School in Attelboro, Massachusetts banning any game incorporating tag.
Principal Gaylene Heppe has approved a ban on playing tag, touch football and other unsupervised chase games, according to The Associated Press. School officials fear that such games make children more vulnerable to injury, thus making the school more vulnerable to lawsuits.Is life to be dictated by lawyers? What are we teaching our children? Life spent quaking (quacking?) behind the threat of litigation is worse, in my view, than permitting such beneficial social activities and learning the lessons of life.
Unstructured play time is incredibly important for our children as confirmed by the American Academy of Pediatrics. Furthermore, the benefits of games like “tag” increases physical activity in our children and helps reduce obesity, too. But beyond the physical benefits, teaching our children what life is about – that competition exists and is part of life – that we cannot always “win” and must learn how to cope when we lose – these are the most important lessons we learn in our formative years, are they not?
I ran today’s Tribune editorial by an expert: my daughter, age 11. “What do you think about this?” I asked her.
“Oh Daddy, that’s nothing. You think that’s bad? Guess what all of our teachers tell us when we want to play Tug-of-War?”
I had no idea.
“We can’t call it that, Daddy.”
“Why not?”
“They think it’s too mean to call it Tug-of-War – we have to call it Tug-of-Peace.”
I couldn’t believe my ears. In our neighborhood, our Great American Public school system no longer condones the term “Tug-of-War” on the playground. The ridiculousness of the re-naming was not lost on my 11-year-old daughter. It is both condescending, patronizing, and disingenuous to her. Unfortunately, it seems “war” now so politically incorrect that we can no longer use the term at our school.
A quick question for our "teachers:"
Are we at "peace" in Iraq?
-Wes
Thursday, October 19, 2006
Curing Angina for the Soul
From my wife in her piece this month for "From the Shrink's Desk" (As a cardiologist, I can identify with this 'anginal equivalent'):
-Wes
I wonder if it’s possible to have angina of the soul. It’s one of those days where I am consumed with restlessness and angst that defies rational logic – but nevertheless, there it is. Having enough years of cognitive therapy to stop a steam engine – I am unable to stop this lonely feeling. The only thing that will help is doing something artistic.I'm grabbing the wine, dear...
So I leave the stacked dishes, the mail pile, the unsorted clean laundry – I leave it all, and begin to arrange fall gourds and pumpkins on the porch. I commit myself to deciding if kale and fall grasses – maybe in a burgundy shade…would give me what I am looking for. I head to the nursery for a bale of hay with the zeal and gravitas of a woman on a mission. And I am. The nursery fall displays are my nitroglycerin, the soul angina eases. Who cares if it makes sense?
If you are a creative or an artist – you know what I am talking about. If you are this person – you have a resource when this soul hunger comes upon you. There is no real answer, is there? Life is hard – knit a sweater. Life is hard – loom a table runner. Really. It comes down to that.
I think how often we push away from going to the apple orchard, walking in the forest preserve, going to the candlelight chamber concert. In other cultures, this soul need is honored. Opera is for the masses, dinner is a long ritual, coffee stretches for hours – why? Because the needs of the soul as it navigates through life are real. And when are they more real than midlife.
There are so many things in life that cannot or will not be solved. So many things that linger – despite our best efforts, despite our brave face and tireless devotion to the cause.
Sometimes the only answer is respect and tenderness for the self. Some might call it surrender. Cinnamon tea, spice scented candles, lower the lights. Put some opera on the stereo. Light the fire.
It’s time.
-Wes
Wednesday, October 18, 2006
Illinois Medical Record Report Card
Seems our Illinois Medical Licensure Board's website scored pretty poorly on Public Citizen's evaluation of data available online for "medical consumers:" scoring 44th of 65 state licensure web sites (some states have separate sites for osteopathic (DO) and medical (MD) doctors) and 38.8 of a possible 100 points.
But given the issues of privacy for physicians, I take issue why people need to know my birthdate (one of their fields needed to score perfectly). Doctors need to be aware the push to expose more of their private lives and personal information is real - and I have never consulted this database in referring a patient to a colleague.
-Wes
The report covered eight categories in determining its grades: types of physician-identifying information, board disciplinary action information, disciplinary actions taken by hospitals, disciplinary actions taken by the federal government (Medicare, Drug Enforcement Administration, and Food and Drug Administration), malpractice information, criminal conviction information, Web Site search capabilities and other information. The survey found a wide range of Web site quality, with very few states providing disciplinary actions other than those taken by the boards themselves. Forty-four of the 65 boards provided none of this external information, thereby losing 40 points on their possible score of 100.All states rankings can be found here.
But given the issues of privacy for physicians, I take issue why people need to know my birthdate (one of their fields needed to score perfectly). Doctors need to be aware the push to expose more of their private lives and personal information is real - and I have never consulted this database in referring a patient to a colleague.
-Wes
Tuesday, October 17, 2006
On the Lighter Side
This fundraiser has, er, balls. You gotta hand it to these guys (from News-Press.com):
-Wes
Addendum:: This post has made me take pause regarding what will be in my giblet gravy for Thanksgiving.... Perhaps the turkeys that "donated" should be given one of these.
“It’s just kinda silly; it really is,” Kit Chamberlain, a festival worker, told the council. The annual festival has raised about $3,000 for the Harry Chapin Food Bank in each of its past three years. The Surf Club, a Beach bar, hosts the quirky event.Glad the title wasn't castrated - it got my attention, and I'm sure it will do the same for many others. I hope they make twice as much this year for their cause!
The testicles, which are deep fried and dipped in a variety of sauces, are what make the festival such a novelty, supporters said. To take that out of its advertisement could affect attendance.
“You get people who use their cell phone to call people and say, you can’t believe what I’m eating,” Chamberlain said.
Their logo — a frightened turkey with his arms over his crossed legs — is a big sell on T-shirts. Farms in North Carolina donate 100 pounds of turkey testicles.
“If it was a breast cancer awareness raise, would they drop the word breast?” asked Chamberlain, who said all festival advertisements have been printed already.
-Wes
Addendum:: This post has made me take pause regarding what will be in my giblet gravy for Thanksgiving.... Perhaps the turkeys that "donated" should be given one of these.
Grab a Cuppa Joe: Grand Rounds is Up
Kim at Emergiblog has once again shown why she is the queen bee that never sleeps by getting up another great round-up of the medical blog-o-sphere's finest after a 12-hour shift. Grap a cup 'o Joe and enjoy...
-Wes
-Wes
McGuire's Exit Strategy
Doctor William McGuire, for all he's done for UnitedHealth (bless his soul) will "retire" (asked to get the *%^$# out) from Unitedhealth with the following:
Now, if that's not enough, it seems he "doubled down" on the options issued. As reported by the Wall Street Journal this AM:
Worse still: no doubt other insurer CEO's have similar deals.
-Wes
- $6.4 million "see-ya-later" fee
- $5.1 million a year for life
- $2.55 million a year for his wife for life should he die before her (and what, exactly, was her role for Unitedhealth?)
- Lifetime health coverage for him and his wife
- Health coverage for his kids until age 25
- Use of his supplied aircraft
- Company-paid office and secretary for three years
- Company-paid "allowance" for tax-planning and financial planning
- Company-paid "allowance" for security
Now, if that's not enough, it seems he "doubled down" on the options issued. As reported by the Wall Street Journal this AM:
The internal report that led to Dr. McGuire's departure gave one example of how options could become so lucrative. The report, by the firm of Wilmer Cutler Pickering Hale & Dorr, described an unusual options swap in which Dr. McGuire and others managed to get the same options twice.Sick. Just sick. That $250,000,000 could fund 25,000 patients's annual health care benefit costs (if one assumes $10,000 per year of fees per patient). Such options transactions hurt our healthcare system and need to be made a felony. Remember, Dr. McGuire: primum non nocere!
In October 1999, the report says, Dr. McGuire suggested in a memo that "employee morale and retention" were being hurt by old options that carried strike prices above the company's then-market price. The board agreed to suspend a total of two million out-of-the-money options and replace them with a similar number of new options, which were priced at the lowest point of the year. The Wilmer report concluded the new options likely were improperly backdated to that low point to give the insiders an extra boost.
By the following August, however, the company's stock price had risen significantly. The board then agreed to reactivate the suspended options. So in effect, Dr. McGuire and the others double-dipped, getting back their original options while also keeping the replacement options.
In Dr. McGuire's case, the Wilmer report found, the maneuver in essence got him an extra 750,000 options, with an instant paper gain of about $26 million. Those options are now valued at about $250 million because of share splits and an increased stock price.
The report also concluded that the company failed to properly disclose and account for the complex transaction.
Worse still: no doubt other insurer CEO's have similar deals.
-Wes
Monday, October 16, 2006
Combination Drugs: Intellectual Property Hogs?
Today it was reported (subscription required) that BiDil, a combination drug of isorsorbide (a nitrate) and hydralazine (an alpha blocker/vasodilator), made by Nitromed, Inc., and specifically approved for use in blacks with congestive heart failure, has had underpenetration of the market due to its high price. Insurers have argued that the other generic medications (isorsorbide and hydralazine) can be administered separately for less cost, explaining the underpenetration in blacks despite significant clinical improvement in heart failure symptoms with the medication.
Now it is rumored that Nitromed may threaten intellectual property infringement if separate drugs are used instead (WSJ):
Intellectual property threats like this only serve to discredit Nitromed, Inc. They might want to rethink this stance.
-Wes
Now it is rumored that Nitromed may threaten intellectual property infringement if separate drugs are used instead (WSJ):
NitroMed, meanwhile, is taking a hardball stance. It says it believes insurers that encourage the prescription of the two generic drugs instead of BiDil may be bordering on patent infringement. That's because the company owns several patents covering the combination use of isosorbide and hydralazine, either as separate pills or in a single pill, for the treatment of heart failure. The company has sent letters to more than a dozen health insurance plans, including Aetna Inc., Humana Inc. and Coventry Health Care Inc., placing them on notice of this view.Give me a break! While I understand the company's concerns about lack of sales, the thought they'd come after me due to intellectual property infringement because I choose to save my patient a few bucks by using separate generic drugs will NEVER fly. Too many other examples of combination drugs are out there and if my patient is willing to take the generics more frequently to save a few buck, so be it!
"We'd much rather have the plans as our customers and we don't want to be litigants," says company spokeswoman Jane Kramer. "But if it becomes necessary to fight for our intellectual property, we will."
Aetna replied that it was "very confident that our actions do not violate any patent rights." A spokeswoman for Humana said she had not been able to find a record confirming receipt of the letter at the health plan. Coventry didn't return several requests for comment.
Intellectual property threats like this only serve to discredit Nitromed, Inc. They might want to rethink this stance.
-Wes
Duke Lacrosse
No matter what one thinks of the Duke Lacrosse scandal (and there is much to say here), it was refreshing to hear the players and one of the strippers tell their story on CBS's 60 minutes last PM. The worst foul of the entire escapade had to be that of DA Mike Nifong's handling of the entire affair. Although it appears from this report that no rape occurred, the effected individuals' lives - all of them - will be forever changed thanks to his Nifong's egregious actions.
-Wes
-Wes
Sunday, October 15, 2006
Medical "Tours"
"Hey doc, I've been having this chest pain when I walk a few feet. It's getting so bad I can barely walk from my bed to the bathroom."
"Really? Hmm. *click* I see from your chart, Mr. Smith, that you don't have health insurance. *click* And you have six kids. *click* But you have been working steadily at McDonalds for the last 10 years. *click* oh, and you have an ample supply of nitroglycerine."
"Yeah."
"Well congratulations, Mr. Smith! You've qualified for an all inclusive Medical Tour to India!" * Tah dah * goes the computer. "Just think: an all-inclusive package with airfare, surgery, un-air-conditioned transportation to and from the medical facility, bottled water, 8 nights of accommodations, and tour of the Taj Mahal, all for the low-low price of $10,812!!"
"But I can't er, walk, too far."
"Oh, now, don't be a party pooper, Mr. Smith. Imagine the opportunity for world travel! There's nothing like flying cheek-to-cheek in economy comfort in the airplane both to and from your destination for the quick 23-hour flight! Isn't that worth the little chest pain you'll get carrying your bags on board? And think of the return trip with those leg wounds you'll have! You know, the ones where they harvest the veins to bypass those nasty little blockages. You'll be the entertainment for your entire row!"
"But my family..."
"There, there, Mr. Smith. Don't worry about them! They'll be so happy you've taken this Tour. After all, you'll be saving them thousands of dollars while basking in the.... er, wait, it's June ... well, the monsoons there won't be too bad. And when was the last time you saw rain like that? I mean, come on, Mr. Smith, be a player!"
"But they won't be there for me...."
"You don't need their support, Mr. Smith, it's just a tiny surgery. No biggie, Mr. Smith. Or, er, I hear they have companion fares if you get an American Express platinum card, Mr. Smith. You know: buy one airfare, get the other one free... can I interest you?" * Holds up the American Express brochure to Mr. Smith *
"Really?"
"Sure! And the best part, Mr. Smith, I've heard your employer will pay you money for taking this trip: they'll give you 20% of the cost savings they receive compared to what it would cost you here in the States! Wouldn't the kids like something special for Christmas?"
"Wow. I had no idea..."
"And that's just the beginning. The cows on the street, the incredible traffic, rickshaws, lack of center lines on the roads, it all makes for one thrilling and entertaining ride to and from the hospital! And the water. Oh, the water there. It's sparkling fresh - from the bottle, of course. But if you're the daring type, heck, try a little of the native water. You're sure to have some fun, then! Oh, but you'll need one more medication."
"What's that?"
"Mefloquine."
"Huh?"
"Just a little something to help with those nasty mosquitos. No big deal, really."
"Thanks, doc." Suddenly, Mr. Smith's chest tightness grows a bit at rest. "Er, doc, I'm having some of that chest pain again."
"Have any of those nitro pills, Mr. Smith? Try throwing one under your tongue, we wouldn't want you disqualified from your trip now, would we?"
"Gosh, no, doc!" Scrambling, he finds his nitroglycerine tablets and pops one under his tongue. Minutes later, he's breathing better. "Thanks, doc."
"Hey, no problem, Mr. Smith. Glad I could help. I mean, who needs medical care when there's Medical Tours! Bon voyage!"
-Wes
"Really? Hmm. *click* I see from your chart, Mr. Smith, that you don't have health insurance. *click* And you have six kids. *click* But you have been working steadily at McDonalds for the last 10 years. *click* oh, and you have an ample supply of nitroglycerine."
"Yeah."
"Well congratulations, Mr. Smith! You've qualified for an all inclusive Medical Tour to India!" * Tah dah * goes the computer. "Just think: an all-inclusive package with airfare, surgery, un-air-conditioned transportation to and from the medical facility, bottled water, 8 nights of accommodations, and tour of the Taj Mahal, all for the low-low price of $10,812!!"
"But I can't er, walk, too far."
"Oh, now, don't be a party pooper, Mr. Smith. Imagine the opportunity for world travel! There's nothing like flying cheek-to-cheek in economy comfort in the airplane both to and from your destination for the quick 23-hour flight! Isn't that worth the little chest pain you'll get carrying your bags on board? And think of the return trip with those leg wounds you'll have! You know, the ones where they harvest the veins to bypass those nasty little blockages. You'll be the entertainment for your entire row!"
"But my family..."
"There, there, Mr. Smith. Don't worry about them! They'll be so happy you've taken this Tour. After all, you'll be saving them thousands of dollars while basking in the.... er, wait, it's June ... well, the monsoons there won't be too bad. And when was the last time you saw rain like that? I mean, come on, Mr. Smith, be a player!"
"But they won't be there for me...."
"You don't need their support, Mr. Smith, it's just a tiny surgery. No biggie, Mr. Smith. Or, er, I hear they have companion fares if you get an American Express platinum card, Mr. Smith. You know: buy one airfare, get the other one free... can I interest you?" * Holds up the American Express brochure to Mr. Smith *
"Really?"
"Sure! And the best part, Mr. Smith, I've heard your employer will pay you money for taking this trip: they'll give you 20% of the cost savings they receive compared to what it would cost you here in the States! Wouldn't the kids like something special for Christmas?"
"Wow. I had no idea..."
"And that's just the beginning. The cows on the street, the incredible traffic, rickshaws, lack of center lines on the roads, it all makes for one thrilling and entertaining ride to and from the hospital! And the water. Oh, the water there. It's sparkling fresh - from the bottle, of course. But if you're the daring type, heck, try a little of the native water. You're sure to have some fun, then! Oh, but you'll need one more medication."
"What's that?"
"Mefloquine."
"Huh?"
"Just a little something to help with those nasty mosquitos. No big deal, really."
"Thanks, doc." Suddenly, Mr. Smith's chest tightness grows a bit at rest. "Er, doc, I'm having some of that chest pain again."
"Have any of those nitro pills, Mr. Smith? Try throwing one under your tongue, we wouldn't want you disqualified from your trip now, would we?"
"Gosh, no, doc!" Scrambling, he finds his nitroglycerine tablets and pops one under his tongue. Minutes later, he's breathing better. "Thanks, doc."
"Hey, no problem, Mr. Smith. Glad I could help. I mean, who needs medical care when there's Medical Tours! Bon voyage!"
-Wes
Saturday, October 14, 2006
Good Riddance, Dr. McGuire
From the Wall Street Journal:
-Wes
"William McGuire, chairman and chief executive of UnitedHealth Group Inc., faces mounting boardroom pressure to leave the giant health insurer after an internal probe found evidence that stock options were improperly backdated to benefit insiders, people familiar with the matter said.It's time to say good-bye.
Dr. McGuire's fate, along with that of general counsel David Lubben, could be decided at a board meeting scheduled to take place Sunday, these people said.
Directors received a detailed briefing on the results of the months-long internal probe Friday in Washington. The probe was conducted by law firm WilmerHale. The meeting included a lengthy presentation by Dr. McGuire and his attorney.
UnitedHealth, one of the nation's largest health insurers with a market value of $66 billion, is among the most prominent of the more than 100 companies caught up in the stock-options scandal. Dr. McGuire has been among the highest-paid executives in U.S. corporate history, amassing an enormous, options-based fortune over his 15 years running UnitedHealth. At the end of 2005, his unexercised cache of options was valued at $1.78 billion, far and away the largest sum held by any U.S. executive, according to Standard & Poor's ExecuComp."
-Wes
Mobile Phones in Hospitals
Finally, the Brits once again demonstrate their common sense. Mobile phones are used in most hospitals all the time, despite warnings posted all over hospitals, and I haven't seen a single patient killed by them - this is especially true with newer digital cellphones. In fact, cell phone use on the ward has been the standard in some hospitals I have worked at for years - their use signficantly improved communication between the doctor and nurse caring for the patient in those facilities.
What I HAVE seen, however, was an event several years ago (1999?) when a high definition TV tower in Cincinnati, OH was activated, it shut down the University Hospital, Cincinnati's entire telemetry unit due to direct interference: not a pretty site. Seems this happened at Baylor and Methodist Hospitals in Houston, TX, and this from a communication from Univeristy of Texas regarding another hospital in Minnesota:
-Wes
What I HAVE seen, however, was an event several years ago (1999?) when a high definition TV tower in Cincinnati, OH was activated, it shut down the University Hospital, Cincinnati's entire telemetry unit due to direct interference: not a pretty site. Seems this happened at Baylor and Methodist Hospitals in Houston, TX, and this from a communication from Univeristy of Texas regarding another hospital in Minnesota:
My wife (PICU RN) confirmed that they don't allow cellular phones on their unit but she doesn't recall problems with radios. Interesting tale from one of their medical bulletins: when a Minnesota station started broadcasting its HDTV signal it disrupted heart monitors (readout only) in the general vicinity of the TV set in one of the rooms or lounges. Don't know what happened to the pacemaker-wearers. TV you could die for!(My note: pacemakers weren't effected.) Funny how we never heard about this in the press.
-Wes
Friday, October 13, 2006
Chili Cook-Off
My wife, in her younger years, was voted as “Chili Queen” from Springfield, IL during one of their annual Chili cook-offs. Today, this e-mail was sent to her by her father in memory of that occasion:
If you can read this whole story without laughing, then there's no hope for you. I was crying by the end. For those of you who have lived in Texas, you know how true this is. They actually have a Chili Cook Off about the time Halloween comes around. It takes up a major portion of a parking lot at the San Antonio City Park. Judge #3 was an inexperienced Chili Taster named Frank, who was visiting from Springfield, IL.
******************************************************
Mark: "Recently, I was honored to be selected as a judge at a chili cook-off. The original person called in sick at the last moment and I happened to be standing here at the judge's table asking for directions to the Coors Light truck, when the call came in. I was assured by the other two judges (Native Texans) that the chili couldn't be all that spicy and, besides, they told me I could have free beer during the tasting, so I accepted."
Here are the scorecard notes from the event:
*****************************************************
CHILI # 1 - MIKE'S MANIAC MONSTER CHILI...
Judge # 1 -- A little too heavy on the tomato. Amusing kick.
Judge #2 - Nice, smooth tomato flavor. Very mild.
Judge # 3 (MARK) -- Holy crap, what the hell is this stuff? You could remove dried paint from your driveway. Took me two beers to put the flames out. I hope that's the worst one. These Texans are crazy.
*****************************************************
CHILI # 2 - AUSTIN 'S AFTERBURNER CHILI...
Judge # 1 -- Smoky, with a hint of pork. Slight jalapeno tang.
Judge #2 -- Exciting BBQ flavor, needs more peppers to be taken seriously.
Judge # 3 -- Keep this out of the reach of children. I'm not sure what I'm supposed to taste besides pain. I had to wave off two people who wanted to give me the Heimlich maneuver. They had to rush in more beer when they saw the look on my face.
*****************************************************
CHILI # 3 - FRED'S BURN DOWN THE BARN CHILI...
Judge # 1 -- Excellent firehouse chili. Great kick.
Judge # 2 -- A bit salty, good use of peppers.
Judge # 3 -- Call the EPA. I've located a uranium spill. My nose feels like I have been snorting Drano. Everyone knows the routine by now. Get me more beer before I ignite. Barmaid pounded me on the back, now my backbone is in the front part of my chest. I'm getting drunk from all of the beer.
*****************************************************
CHILI # 4 - BUBBA'S BLACK MAGIC...
Judge # 1 -- Black bean chili with almost no spice. Disappointing.
Judge # 2 -- Hint of lime in the black beans. Good side dish for
fish or other mild foods not much of a chili.
Judge # 3 -- I felt something scraping across my tongue, but was unable to taste it. Is it possible to burn out taste buds? Sally, the beermaid, was standing behind me with fresh refills. That 300-LB woman is starting to look HOT. just like this nuclear waste I'm eating! Is chili an aphrodisiac?
*****************************************************
CHILI # 5 LISA'S LEGAL LIP REMOVER...
Judge # 1 -- Meaty, strong chili. Cayenne peppers freshly ground,
adding considerable kick. Very impressive.
Judge # 2 -- Chili using shredded beef, could use more tomato. Must admit the cayenne peppers make a strong statement.
Judge # 3 -- My ears are ringing, sweat is pouring off my forehead and I can no longer focus my eyes. I farted and four people behind me needed paramedics. The contestant seemed offended when I told her that her chili had given me brain damage. Sally saved my tongue from bleeding by pouring beer directly on it from the pitcher. I wonder if I'm burning my lips off. It really ticks me off that the other judges asked me to stop screaming.
*****************************************************
CHILI # 6 - VERA'S VERY VEGETARIAN VARIETY...
Judge # 1 -- Thin yet bold vegetarian variety chili. Good balance of
spices and peppers.
Judge # 2 -- The best yet. Aggressive use of peppers, onions, and garlic. Superb.
Judge # 3 -- My intestines are now a straight pipe filled with gaseous, sulfuric flames. I pooped on myself when I farted and I'm worried it will eat through the chair No one seems inclined to stand behind me except that Sally. Can't feel my lips anymore. I need to wipe my ass with a snow cone.
*****************************************************
CHILI # 7 - SUSAN'S SCREAMING SENSATION CHILI...
Judge # 1 -- A mediocre chili with too much reliance on canned peppers.
Judge # 2 -- Ho hum, tastes as if the chef literally threw in a can of chili peppers at the last moment. **I should take note that I am worried about Judge # 3. He appears to be in a bit of distress as he is cursing uncontrollably.
Judge # 3 -- You could put a grenade in my mouth, pull the pin, and I wouldn't feel a thing. I've lost sight in one eye, and the world sounds like it is made of rushing water. My shirt is covered with chili, which slid unnoticed out of my mouth. My pants are full of lava to match my shirt. At least during the autopsy, they'll know what killed me. I've decided to stop breathing it's too painful. I'm not getting any oxygen anyway. If I need air, I'll just suck it in through the 4-inch hole in my stomach.
*****************************************************
CHILI # 8 - BIG TOM'S TOENAIL CURLING CHILI...
Judge # 1 -- The perfect ending, this is a nice blend chili. Not too
bold but spicy enough to declare its existence.
Judge # 2 – This final entry is a good, balanced chili. Neither mild nor hot. Sorry to see that most of it was lost when Judge #3 farted, passed out, fell over and pulled the chili pot down on top of himself. Not sure if he's going to make it. poor feller, wonder how he'd have reacted to really hot chili?
Judge # 3 - No Report
Warning: Spelling errors in this message are the product of a poor school system.
Pay teachures more than athletes.
Have a great weekend! Happy Friday the 13th!
-Wes
If you can read this whole story without laughing, then there's no hope for you. I was crying by the end. For those of you who have lived in Texas, you know how true this is. They actually have a Chili Cook Off about the time Halloween comes around. It takes up a major portion of a parking lot at the San Antonio City Park. Judge #3 was an inexperienced Chili Taster named Frank, who was visiting from Springfield, IL.
******************************************************
Mark: "Recently, I was honored to be selected as a judge at a chili cook-off. The original person called in sick at the last moment and I happened to be standing here at the judge's table asking for directions to the Coors Light truck, when the call came in. I was assured by the other two judges (Native Texans) that the chili couldn't be all that spicy and, besides, they told me I could have free beer during the tasting, so I accepted."
Here are the scorecard notes from the event:
*****************************************************
CHILI # 1 - MIKE'S MANIAC MONSTER CHILI...
Judge # 1 -- A little too heavy on the tomato. Amusing kick.
Judge #2 - Nice, smooth tomato flavor. Very mild.
Judge # 3 (MARK) -- Holy crap, what the hell is this stuff? You could remove dried paint from your driveway. Took me two beers to put the flames out. I hope that's the worst one. These Texans are crazy.
*****************************************************
CHILI # 2 - AUSTIN 'S AFTERBURNER CHILI...
Judge # 1 -- Smoky, with a hint of pork. Slight jalapeno tang.
Judge #2 -- Exciting BBQ flavor, needs more peppers to be taken seriously.
Judge # 3 -- Keep this out of the reach of children. I'm not sure what I'm supposed to taste besides pain. I had to wave off two people who wanted to give me the Heimlich maneuver. They had to rush in more beer when they saw the look on my face.
*****************************************************
CHILI # 3 - FRED'S BURN DOWN THE BARN CHILI...
Judge # 1 -- Excellent firehouse chili. Great kick.
Judge # 2 -- A bit salty, good use of peppers.
Judge # 3 -- Call the EPA. I've located a uranium spill. My nose feels like I have been snorting Drano. Everyone knows the routine by now. Get me more beer before I ignite. Barmaid pounded me on the back, now my backbone is in the front part of my chest. I'm getting drunk from all of the beer.
*****************************************************
CHILI # 4 - BUBBA'S BLACK MAGIC...
Judge # 1 -- Black bean chili with almost no spice. Disappointing.
Judge # 2 -- Hint of lime in the black beans. Good side dish for
fish or other mild foods not much of a chili.
Judge # 3 -- I felt something scraping across my tongue, but was unable to taste it. Is it possible to burn out taste buds? Sally, the beermaid, was standing behind me with fresh refills. That 300-LB woman is starting to look HOT. just like this nuclear waste I'm eating! Is chili an aphrodisiac?
*****************************************************
CHILI # 5 LISA'S LEGAL LIP REMOVER...
Judge # 1 -- Meaty, strong chili. Cayenne peppers freshly ground,
adding considerable kick. Very impressive.
Judge # 2 -- Chili using shredded beef, could use more tomato. Must admit the cayenne peppers make a strong statement.
Judge # 3 -- My ears are ringing, sweat is pouring off my forehead and I can no longer focus my eyes. I farted and four people behind me needed paramedics. The contestant seemed offended when I told her that her chili had given me brain damage. Sally saved my tongue from bleeding by pouring beer directly on it from the pitcher. I wonder if I'm burning my lips off. It really ticks me off that the other judges asked me to stop screaming.
*****************************************************
CHILI # 6 - VERA'S VERY VEGETARIAN VARIETY...
Judge # 1 -- Thin yet bold vegetarian variety chili. Good balance of
spices and peppers.
Judge # 2 -- The best yet. Aggressive use of peppers, onions, and garlic. Superb.
Judge # 3 -- My intestines are now a straight pipe filled with gaseous, sulfuric flames. I pooped on myself when I farted and I'm worried it will eat through the chair No one seems inclined to stand behind me except that Sally. Can't feel my lips anymore. I need to wipe my ass with a snow cone.
*****************************************************
CHILI # 7 - SUSAN'S SCREAMING SENSATION CHILI...
Judge # 1 -- A mediocre chili with too much reliance on canned peppers.
Judge # 2 -- Ho hum, tastes as if the chef literally threw in a can of chili peppers at the last moment. **I should take note that I am worried about Judge # 3. He appears to be in a bit of distress as he is cursing uncontrollably.
Judge # 3 -- You could put a grenade in my mouth, pull the pin, and I wouldn't feel a thing. I've lost sight in one eye, and the world sounds like it is made of rushing water. My shirt is covered with chili, which slid unnoticed out of my mouth. My pants are full of lava to match my shirt. At least during the autopsy, they'll know what killed me. I've decided to stop breathing it's too painful. I'm not getting any oxygen anyway. If I need air, I'll just suck it in through the 4-inch hole in my stomach.
*****************************************************
CHILI # 8 - BIG TOM'S TOENAIL CURLING CHILI...
Judge # 1 -- The perfect ending, this is a nice blend chili. Not too
bold but spicy enough to declare its existence.
Judge # 2 – This final entry is a good, balanced chili. Neither mild nor hot. Sorry to see that most of it was lost when Judge #3 farted, passed out, fell over and pulled the chili pot down on top of himself. Not sure if he's going to make it. poor feller, wonder how he'd have reacted to really hot chili?
Judge # 3 - No Report
Warning: Spelling errors in this message are the product of a poor school system.
Pay teachures more than athletes.
Have a great weekend! Happy Friday the 13th!
-Wes
Why Doctors Resist the EMR
( Cartoon from Jerry Scott and Jim Borgman, "Random Zits," Andrews McNeal Publishing, 2004)
Top Ten Reasons Electronic Medical Records Aren’t Catching On With Doctors
10) Privacy concerns and concerns about controlling access to records
9) Cost
8) Inability to archive and retrieve graphical information (EKG's, rhythm strips, photos, etc.)
7) Computer system obsolescence and need for renewed investment later
6) Lack in system interconnectivity and the continued need for redundant data entry across platforms.
5) Time for data entry
4) Pay for Performance and its implementation using the EMR (A must-read example: via Dr. Rant)
3) Docotes caoifg thyk
2) Soxters can”t t7pe
1) Doctors can’t type!
- Wes
Thursday, October 12, 2006
New St. Jude Pacemaker Advisory
Tomorrow doctors will receive a "Dear Doctor" letter notifying them about a software problem with St. Jude Medical's Identity SR, Identity DR, and Identity XL DR pacemakers. This advisory was issued because of 53 reports or 0.027% (of 199,100 devices) where the patient's elective replacement indicator (ERI) measurement that was stored in the memory of the device was "frozen." This problem might lead the physician to think that acceptable battery voltage remained in the device. However, if a second, real-time measurement is performed, the ACTUAL battery voltage and longevity estimate will be correctly displayed.
Fortunately, the problem can be corrected with an injected software fix (no surgery required). The software, we are told, should be available in about two months. Patients with these devices should check with their doctor during their routine pacemaker checks to assure they receive the newest software installed on their device when it becomes available.
-Wes
Fortunately, the problem can be corrected with an injected software fix (no surgery required). The software, we are told, should be available in about two months. Patients with these devices should check with their doctor during their routine pacemaker checks to assure they receive the newest software installed on their device when it becomes available.
-Wes
Wednesday, October 11, 2006
Standing US Healthcare on Its Ear
When health care costs are 80% cheaper, should employers ship their employees overseas?
Scary thing is, it seems if the medical liability concerns are resolved, this will be a whole "new world" in healthcare.
I just hope I don't have to go to Dehli for my ulcer treatment when this becomes reality.
-Wes
Mr. Garrett, who works for Blue Ridge Paper Products in Canton, N.C., had volunteered to get his treatments in India in return for a share in the company’s savings. Blue Ridge now says it will find Mr. Garrett a treatment alternative in the United States and will offer the overseas option only to its salaried employees.I had no idea there were companies like IndUShealth out there. But after looking into their hospital partners and recalled I had been to Escorts Heart Institute in Dehli - a relatively modern facility that catered to the more affluent population in India. I was there in 2001 as a "physician trainer" for Medtronic's launch of the Insync biventricular pacemaker for the treatment of patients with heart failure (at the time they didn't do heart transplants there -- too expensive). The facility was, er, nice (especially relative to the local government facility), but certainly not to the standard of US hospitals. It scares me that cost alone (and how they're going to sue if one of their employees has a complication) is what matters to US businesses.
IndUShealth, a company based in North Carolina that arranges health care in India for Americans, would have made Mr. Garrett’s medical arrangements. The company acknowledged that its plan to send Blue Ridge workers to India was “on hold” but said it was exploring deals with other employers.
Scary thing is, it seems if the medical liability concerns are resolved, this will be a whole "new world" in healthcare.
I just hope I don't have to go to Dehli for my ulcer treatment when this becomes reality.
-Wes
Tuesday, October 10, 2006
Transcatheter Aortic Valve Debuts in Man
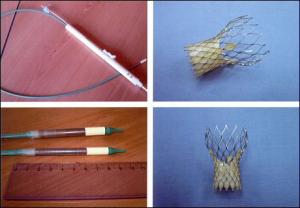
As reported from TheHeart.org:
Percutaneous implantation of the self-expanding CoreValve aortic valve bioprosthesis in the first-ever series of patients shows that the procedure is feasible in those deemed too high risk for valve surgery and, when successful, results in marked hemodynamic and clinical improvement at 30 days [1].The lessons learned included:
However, there was a high periprocedural mortality of 20%, and there are several important lessons to be learned from this first-in-human single-center study, say the researchers, led by Dr Eberhard Grube (HELIOS Heart Center, Siegburg, Germany). They report their findings in the October 10, 2006 issue of Circulation.
- From TheHeart.org:
First, the periprocedural morality was high (five of the 25 patients died). Two patients died of procedure-related events (one from wire perforation of the left ventricle, one after the inability of the prosthesis to cross a heavily calcified valve). A third patient was not pretreated with clopidogrel and died of disseminated intravascular coagulation, while two others who also did not receive a thienopyridine before the implant developed a severe thrombocytopenia of prolonged duration.
- Surgery in the type of patients studied often carried operative mortalities as high as 50%
- Extracorporeal circulatory support was used in the early phase of the trial and that this could have contributed to complications (Especially thrombocytopenia - a low blood product count called platelets that can lead to severe bleeding.
- The optimal antiplatelet and antithrombotic (blood thinning) regimen to support implantation of the CoreValve device needs to be clarified
- The precise positioning of the device "remains challenging and was responsible for half the procedural failures. In this regard, the role of transesophageal echocardiography to guide placement continues to evolve, and markers are being added to the device to facilitate accurate positioning."
- Larger device sizes need to accommodate men's larger aortic sizes.
It's too early to know if this self-expanding design will supplant or complement the balloon-delivered aortic valve replacement called the Edwards Life Sciences Aortic PHV device but it is a courageous start.
-Wes
[1] Reference: Grube E, Laborde JC, Gerckens U, et al. Percutaneous implantation of the CoreValve self-expanding valve prosthesis in high-risk patients with aortic valve disease. The Siegburg first-in-man study. Circulation 2006; 114: 1616-1624.
Grand Rounds - Vol 3, No. 3
Grand rounds is up at Unbounded Medicine. Jon Mickel, MD did a nice job on a simple, organized approach to the best of the medical blog-so-sphere.
--Wes
--Wes
Monday, October 09, 2006
Your Distributed Medical Record
With the increased sophistication of implantable medical devices, an interesting area of health care law is likely to be tested: who holds and is responsible for your health care data?
This issue came to light recently as we have struggled to integrate electronic information downloaded from pacemakers and defibrillators into the patient’s medical record. As I have discussed before, the Center for Medicare and Medicaid Services has agreed to reimburse physicians for the evaluation of data from pacemaker and defibrillator interrogations. But the patient uploads their information to a “server” owned by a company (usually the manufacturer of that device or their designated company). The server then compiles the information for the physician to review. Easy enough.
But CMS requires the graphical information be preserved from the EKG portion of the interrogation to verify billing. As such, this graphical information does not easily transport from one computer system to another. So it stays on the company’s server.
But sometimes we might need that data later, especially in the case of a medical malpractice claim or to verify a bill. Years later, could we get this interrogation data? Perhaps, if we had stored an electronic or paper copy of the original interrogation locally and saved it on our server. But more and more, it seems the medical device companies will also have this data as backup. So I ask, who is responsible for protecting your medical data?
I believe this issue will become more and more common as the era of the electronic medical record takes hold. Your Electronic Medical Record (EMR) will soon be housed in more than one location - a distributed electronic medical record, if you will. But the issues of responsibility for that data, especially in terms of potential liability claims, will remain murky.
Sounds like the old “file-sharing” system like that of the original Napster music sharing web-site – a modified “peer-to-peer” model of the Electronic Medical Record, eh? But will the individual patient be like the Music Industry executives and prevent our “copyrighted” (well, at least private) sensitive medical information to be similarly restricted in its distribution?
I doubt it. The era of EMR “file-sharing” has arrived.
--Wes
This issue came to light recently as we have struggled to integrate electronic information downloaded from pacemakers and defibrillators into the patient’s medical record. As I have discussed before, the Center for Medicare and Medicaid Services has agreed to reimburse physicians for the evaluation of data from pacemaker and defibrillator interrogations. But the patient uploads their information to a “server” owned by a company (usually the manufacturer of that device or their designated company). The server then compiles the information for the physician to review. Easy enough.
But CMS requires the graphical information be preserved from the EKG portion of the interrogation to verify billing. As such, this graphical information does not easily transport from one computer system to another. So it stays on the company’s server.
But sometimes we might need that data later, especially in the case of a medical malpractice claim or to verify a bill. Years later, could we get this interrogation data? Perhaps, if we had stored an electronic or paper copy of the original interrogation locally and saved it on our server. But more and more, it seems the medical device companies will also have this data as backup. So I ask, who is responsible for protecting your medical data?
I believe this issue will become more and more common as the era of the electronic medical record takes hold. Your Electronic Medical Record (EMR) will soon be housed in more than one location - a distributed electronic medical record, if you will. But the issues of responsibility for that data, especially in terms of potential liability claims, will remain murky.
Sounds like the old “file-sharing” system like that of the original Napster music sharing web-site – a modified “peer-to-peer” model of the Electronic Medical Record, eh? But will the individual patient be like the Music Industry executives and prevent our “copyrighted” (well, at least private) sensitive medical information to be similarly restricted in its distribution?
I doubt it. The era of EMR “file-sharing” has arrived.
--Wes
Sunday, October 08, 2006
Chocolate Chip Cookies for High Cholesterol?
I've been wondering who forms the Institute of Medicine. You know, those same guys who want Pay for Performance for doctors and want to rid the world of all those 5 gazillion annual medical errors out there, lurking around every corner: the same guys cited by credible sources in the Halls of Congress, New York Times, Washington Post, and the Associated Press.
I think I found it. I was just trying to learn about chocolate chip cookies for your high cholesterol. "Bravo!" I thought, "I can't wait until my obese, diabetic patients bring me a bag of these."
But before you go out and buy them, look a bit closer. The study referenced was in a whopping 33 patients and was reported in the Journal of Nutrition. (I could not find mention of conflicts of interest of the authors either, but I digress). Now, if one looks at the nutritional value of just 1 tablespoon of chocolate chips, one can see that those little chocolate chips represent 80 calories, 40 of which are from the 4.5 grams of fat, over half of which (2.5 grams) are saturated fats. Blood cholesterol levels, my friends, are closely related to the amount of saturated fat in one's diet.
So to find that the "study" cookies had 6 grams of fat per cookie (1.9g saturated) and the "placebo" cookie had 7.6 grams of fat (2.2g saturated) was quite a surprise. Now I don't know about you, but shouldn't the placebo cookie have had the same amount of fat? What a clever way to skew the results!
Now, if these guys were really about lowering cholesterol, they'd leave out the chocolate chips, but that might make the cookies taste like cardboard. But given the study was sponsored by RD Foods, the study cookie's manufacturer, one shouldn't be surprised. It seems, too, that one of the authors, John H. Contois, was from Liposcience, Inc. of Raleigh, NC. Interesting that Liposcience's chairman of the board, Charles A Sanders, MD is also a member of the infamous Institute of Medicine that makes all the proclamations about "errors" in medicine.
I wonder if the Institute of Medicine ever considered the errors they help promote in healthcare when their members' companies support these "studies" with pure profit motives.
-Wes
I think I found it. I was just trying to learn about chocolate chip cookies for your high cholesterol. "Bravo!" I thought, "I can't wait until my obese, diabetic patients bring me a bag of these."
But before you go out and buy them, look a bit closer. The study referenced was in a whopping 33 patients and was reported in the Journal of Nutrition. (I could not find mention of conflicts of interest of the authors either, but I digress). Now, if one looks at the nutritional value of just 1 tablespoon of chocolate chips, one can see that those little chocolate chips represent 80 calories, 40 of which are from the 4.5 grams of fat, over half of which (2.5 grams) are saturated fats. Blood cholesterol levels, my friends, are closely related to the amount of saturated fat in one's diet.
So to find that the "study" cookies had 6 grams of fat per cookie (1.9g saturated) and the "placebo" cookie had 7.6 grams of fat (2.2g saturated) was quite a surprise. Now I don't know about you, but shouldn't the placebo cookie have had the same amount of fat? What a clever way to skew the results!
Now, if these guys were really about lowering cholesterol, they'd leave out the chocolate chips, but that might make the cookies taste like cardboard. But given the study was sponsored by RD Foods, the study cookie's manufacturer, one shouldn't be surprised. It seems, too, that one of the authors, John H. Contois, was from Liposcience, Inc. of Raleigh, NC. Interesting that Liposcience's chairman of the board, Charles A Sanders, MD is also a member of the infamous Institute of Medicine that makes all the proclamations about "errors" in medicine.
I wonder if the Institute of Medicine ever considered the errors they help promote in healthcare when their members' companies support these "studies" with pure profit motives.
-Wes
Saturday, October 07, 2006
A Find
Some times, God sends you the coolest things. While raking, a friend happened along my way, and posed for a few shots:



He was nearly six inches long and a beautiful specimen, indeed!
Addendum 10:30PM: Reminds me of a New Yorker Magazine cartoon I was given by a friend from 4 Feb 2002 (thanks to Bill):
Isn't that just like life? You have to take the good with the bad... :)
--Wes



He was nearly six inches long and a beautiful specimen, indeed!
Addendum 10:30PM: Reminds me of a New Yorker Magazine cartoon I was given by a friend from 4 Feb 2002 (thanks to Bill):

Isn't that just like life? You have to take the good with the bad... :)
--Wes
Decision Trees
 “How do I decide?”
“How do I decide?”I asked him as I tried to decipher the myriad of college choices in my earlier years. The choices, even then, were mind-boggling. How to decide your college – was it by location, cost, number of professors with PhD’s? How, oh, how does one decide? I asked again:
“Seriously, how does one decide?”
“Make a list,” he said. “Make it as big as you need it to be, and make a chart with attributes as the columns and the different schools as the rows. Then fill it in and use this to make your decision. No one ever said this was going to be easy…”
And so I did. Suddenly the fifty colleges were weaned to three. Although the list concept hasn’t final, it had helped narrow the choices. I had a better grasp of the situation and the chart helped me decide on my college to attend.
So it was with a bit of reservation that I decided to help with another much more difficult situation. How does one decide to proceed with medical therapies when life has gotten so much tougher to cope. Call it frailty, call it aging, call it whatever you’d like: getting older can be tough, even for the heartiest of minds. Perhaps particularly for those hearty of mind.
“Your left kidney doesn’t work at all, and your right kidney, well that one works a bit, but its function is very marginal.”
“So what are the options?”
“Well, …” and I proceeded to recite the options for him in detail. Each possible option and test, each permutation of possible outcomes described in as simple terms as I could generate. Slowly. Meticulously. He sat in quietly, thinking, eyes looking away. He seemed lost, alone, frustrated, sad, confused.
“Could you go over that again?”
Again? How could he want me to go over that again? I couldn’t have been clearer. At least so I thought. But looking at him then, seeing the sadness and frustration at not being able to control his destiny, that’s when I realized that it was not about his options. It was about him listening, studying, spending time with those he trusted and loved. The noise of illness had clouded his head. It was all-consuming for him: too important to breeze by. It was stay and fight or retreat. In essence, about life or death.
So I drew him a drawing, and then a chart and decision tree. Just like the chart he had help me construct in an earlier time. “If you do this, then one of two things will happen. At each of those points, another decision,” and so on. He stopped and looked at the drawing.
“So down this way, I might feel better.”
“Yep,” I said.
“And these other ways?”
‘They might lead to either more tests or even tougher decisions…” I left it at that. I couldn’t work down every path with him, instead I focused on the optimistic routes. It’s tough when you know too much as a doctor.
He understood.
Life is a journey that begins with birth and ends with death. Once we start on that journey, it never stops. He had made a million decisions in his lifetime, traveled down many highways with forks in the road and made the best of the road he traveled. But his journey was nearing its end and the decisions have become fewer, but no less challenging with each new twist of fate. I had drawn his map for now, but he, alone, had chosen his path again. Gratefully, he had the faculties to help make some of these decisions. Gratefully, I had the fortune of being able to help him just as he had helped me before.
And like a million other times, he forged forward, scheduled an appointment to do what he knew had to be done: my mentor once again.
--Wes
Photo credit: Rolanda Adams
Friday, October 06, 2006
More Pharmaceutical SleezeBags
Seems First DataBank's quiet move to raise pharmacy profits was thwarted by a lawsuit filed by the New England Regional Council of Carpenters. As reported in the Wall Street Journal this AM:
--Wes
First DataBank doesn't buy or sell drugs -- it publishes lists of drug prices. Health plans and state Medicaid programs use those prices as a benchmark in determining what they pay pharmacies.They should have to pay more, much more, than the 5% rollback in published prices. Somehow the sleezebags always seem to get their way....
If the benchmark goes up, so do costs for these payers. That's what happened in 2002, when First DataBank suddenly made broad revisions to its key published list. The new prices had the effect of fattening the profits of pharmacies, out of the view of patients and companies who pay for the soaring cost of health care.
A 2002 email by a manager at one of the nation's largest drug wholesalers, San Francisco-based McKesson Corp., describes how pharmacies would be able to more than double their profit for dispensing the cholesterol drug Lipitor and adds, "that is awesome!!"
Now a tentative legal settlement, reached quietly this week in a Boston court, could reduce annual U.S. drug costs by billions of dollars. An economist hired by the plaintiffs puts the savings in 2007 alone at $4 billion. The actual amount could be lower if pharmacies negotiate higher fees to make up for what they are losing.
In the settlement, which is awaiting approval by a judge, First DataBank, of San Bruno, Calif., agrees to reduce many of the prices on its published list by five percentage points. It denies any wrongdoing and isn't paying any damages to the plaintiffs.
--Wes
E-mail Blues
People seemed amazed that doctors don't use e-mail. Well, we do. But this doctor prefers NOT to use it for direct patient care. Why?
Because I can't check it 24/7/365. I do procedures. Some last hours in duration. Or I might be gone for the weekend - and guess what - some places I go do not have Internet access! I had one time early in my career and earlier in the days of e-mail that made me pause.
He was a young man with hypertrophic cardiomyopathy (a genetic disorder that caused his heart muscle to the thickened and prone to potential life-threatening arrhythmias) discovered on a routine physical exam while he (and I) was in the Navy. One day, unbeknownst to me, he nearly fainted while taking a drink from a water fountain. It was innocent enough, he thought. But he decided to drop me an e-mail and mentioned the experience. I didn't expect such a note to land in my e-mail inbox. I learned then that there are problems that arise in some patients' illnesses that demand immediate attention, but they may not realize that their symptoms of, say, intermittent lightheadedness might be a BIG DEAL. Instead, they leave a "little message" in my in box that I discover (to my horror) amongst the sea of spam and administrative e-mails. Fortunately for this gentleman, there was not an undue delay, but I realized after this interaction that all it might take is one missed e-mail in my line of work and the result could be catastrophic.
That's why we have an answering service 24/7/365. That's my we have call schedules to assure a doctor is available, always.
And on a personal side, I try to have a family life outside my "day job." E-mail, like pagers, is an incredible technology that can reach us whereever we go (how many of us have been paged in the bathroom?), but it has its downside. While many of us want to be omnipresent for our patients, there also comes a time where we need a break (Vacation? What's that?). If I logged on each morning to check my e-mail and attended to the latest round of problems on vacation, I wouldn't be on vacation, would I?
E-mail doesn't give anyone a break. Messages just sit in your "inbox" ready to pounce on you when you return.
I laugh at executives in the business world who feel e-mail is efficient as they wade through their 200-500 e-mails a day. Yes, Virginia, information overload exists in the electronic era. And don't get me started about spam...
E-mail is not bad for many routine things in health care, like refill requests and the like. But it takes time each day to empty my "inbox" of all that spam, "informational administrative" e-mail blasts, and well-meaning CME postings from the 300 other divisions in the hospital that I really have no interest in. The time it takes to delete all those e-mails I'd rather be devoting to patient care.
So for now, I'll stick with the old fashioned land-line and personal interaction. Anyone else have thoughts here?
--Wes
Because I can't check it 24/7/365. I do procedures. Some last hours in duration. Or I might be gone for the weekend - and guess what - some places I go do not have Internet access! I had one time early in my career and earlier in the days of e-mail that made me pause.
He was a young man with hypertrophic cardiomyopathy (a genetic disorder that caused his heart muscle to the thickened and prone to potential life-threatening arrhythmias) discovered on a routine physical exam while he (and I) was in the Navy. One day, unbeknownst to me, he nearly fainted while taking a drink from a water fountain. It was innocent enough, he thought. But he decided to drop me an e-mail and mentioned the experience. I didn't expect such a note to land in my e-mail inbox. I learned then that there are problems that arise in some patients' illnesses that demand immediate attention, but they may not realize that their symptoms of, say, intermittent lightheadedness might be a BIG DEAL. Instead, they leave a "little message" in my in box that I discover (to my horror) amongst the sea of spam and administrative e-mails. Fortunately for this gentleman, there was not an undue delay, but I realized after this interaction that all it might take is one missed e-mail in my line of work and the result could be catastrophic.
That's why we have an answering service 24/7/365. That's my we have call schedules to assure a doctor is available, always.
And on a personal side, I try to have a family life outside my "day job." E-mail, like pagers, is an incredible technology that can reach us whereever we go (how many of us have been paged in the bathroom?), but it has its downside. While many of us want to be omnipresent for our patients, there also comes a time where we need a break (Vacation? What's that?). If I logged on each morning to check my e-mail and attended to the latest round of problems on vacation, I wouldn't be on vacation, would I?
E-mail doesn't give anyone a break. Messages just sit in your "inbox" ready to pounce on you when you return.
I laugh at executives in the business world who feel e-mail is efficient as they wade through their 200-500 e-mails a day. Yes, Virginia, information overload exists in the electronic era. And don't get me started about spam...
E-mail is not bad for many routine things in health care, like refill requests and the like. But it takes time each day to empty my "inbox" of all that spam, "informational administrative" e-mail blasts, and well-meaning CME postings from the 300 other divisions in the hospital that I really have no interest in. The time it takes to delete all those e-mails I'd rather be devoting to patient care.
So for now, I'll stick with the old fashioned land-line and personal interaction. Anyone else have thoughts here?
--Wes
Thursday, October 05, 2006
Transcatheter Pulmonary Valve Gets European Approval
 Medtronic announced CE Mark approval for its transcatheter pulmonary valve replacement technology in Europe today. From their press release:
Medtronic announced CE Mark approval for its transcatheter pulmonary valve replacement technology in Europe today. From their press release:Transcatheter valve technology represents a less invasive means to treat heart valve disease and is designed to allow physicians to deliver replacement valves via a catheter through the body’s cardiovascular system, thus eliminating the need to open the chest. Traditionally, open heart surgery has been required to correct the problem and it is not unusual for a patient to undergo multiple, open-heart surgeries during their lifetime. Patients with this condition tire very easily, as the heart over-exerts itself trying to get oxygenated blood throughout the body.Look for more and more trancatheter valve replacement technologies to enter the field of cardiology soon. Aortic valve replacement technologies, mitral valve repair technologies, and others are also on the horizon. Cardiothoracic surgeons aren't happy about these, but the need to repair failed implants will still exist as these devices gain popularity.
Medtronic has partnered with Professor Philipp Bonhoeffer, professor and chief of cardiology and director of the Catheterization Laboratory, Great Ormond Street Hospital for Children (GOSH) in London, and NuMed, a pediatric catheter company in the development of the Melody Valve and Ensemble System. A pioneer in transcatheter valve technology, Professor Bonhoeffer implanted the world’s first transcatheter valve in September 2000. To date, more than 150 patients worldwide have been implanted with the Melody Transcatheter Pulmonary Valve.
CE Mark Approval gives Medtronic the ability to train and educate physicians in Europe in preparation for implanting the Melody™ and Ensemble™ System so that more patients can benefit from this innovative treatment. With proper training in place, Medtronic will work with hospitals across Europe in gaining access to this new technology.
--Wes
Wednesday, October 04, 2006
Change of Shift - The Nursing Blog Carnival - Vol 1, No 8

This week's Change of Shift, the Nursing Blog Carnival, is hosted by Kim at Emergiblog. Check it out for some of the best in nurses' blog postings.
-Wes
Screening Athletes for Sudden Cardiac Death
There are few things that make me more anxious than the evaluation of the competitive athlete for their risk of sudden cardiac death. There have been many instances of famous athletes collapsing on the basketball court or football field – suddenly and unexpectedly. Every one of these tragic events seems to occur with a host of witnesses and often lands on the front page of the local newspaper. The stakes are high for all involved. To deny an athlete the opportunity to play can be catastrophic to the athlete, while permitting an athlete to play and having them die can be equally (if not more) catastrophic to the physician and the surviving family members.
Today a large population-based observational study from Italy regarding the potential benefits of screening athletes for their risk of cardiovascular death was published in the Journal of the American Medical Association. This study compiled the incidence of cardiovascular death in athletic and non-athletic individuals between 12 and 35 years of age between 1979 and 2004 in the Veneto region of Italy. After 1982 all participants in competitive sports were required by Italian law to undergo screening for cardiovascular diseases at risk of sudden death during sports. Their evaluation included a family and personal history, physical examination and electrocardiogram (ECG). The findings of the large study demonstrated that there were 55 deaths in the screened athletes compared to 265 deaths in unscreened non-athletes, and the incidence of death decreased from 1 in 27,777 athletes to 1 death in 250,000 athletes over the period studied, an 89% reduction. The presence of an ECG in the screening criteria differs from the current recommendations by the American Heart Association, but is in line with the recommendations of the Sports Cardiology Study Group of the European Society of Cardiology.
Now before leaping to conclusions, there were some significant limitations to this study, many of which were nicely outlined by Paul Thompson, MD and Benjamin Levine, MD in their accompanying editorial published in the same issue. They include:
But one thing seems clear to me. An ECG is a remarkably simple and non-invasive test to evaluate the heart. Right ventricular abnormalities, chamber enlargement or ventricular hypertrophy, abnormal electrical pathways (Wolff-Parkinson-White syndrome), repolarization abnormalities (congenital Long QT Syndrome) and arrhythmias can be readily detected. Physical examination often cannot detect these subtle killers. And while this study is not conclusive and has significant limitations, it serves as the most potent longitudinal study to date of the value of screening to prevent death in our young athletes.
The addition of the ECG to screening of athletes, given this study’s data, should be seriously considered. For a small cost, It might just save a young athlete’s life and keep me off the front page of the Chicago Tribune.
-Wes
Today a large population-based observational study from Italy regarding the potential benefits of screening athletes for their risk of cardiovascular death was published in the Journal of the American Medical Association. This study compiled the incidence of cardiovascular death in athletic and non-athletic individuals between 12 and 35 years of age between 1979 and 2004 in the Veneto region of Italy. After 1982 all participants in competitive sports were required by Italian law to undergo screening for cardiovascular diseases at risk of sudden death during sports. Their evaluation included a family and personal history, physical examination and electrocardiogram (ECG). The findings of the large study demonstrated that there were 55 deaths in the screened athletes compared to 265 deaths in unscreened non-athletes, and the incidence of death decreased from 1 in 27,777 athletes to 1 death in 250,000 athletes over the period studied, an 89% reduction. The presence of an ECG in the screening criteria differs from the current recommendations by the American Heart Association, but is in line with the recommendations of the Sports Cardiology Study Group of the European Society of Cardiology.
Now before leaping to conclusions, there were some significant limitations to this study, many of which were nicely outlined by Paul Thompson, MD and Benjamin Levine, MD in their accompanying editorial published in the same issue. They include:
- The study was not a controlled comparison of the screening versus non-screening of athletes, but rather a population-based observational study.
- The study did not evaluate the routine use of ECGs compared with more limited screening based on just history and physical examination.
- There are differences in disease prevalence in Italy versus the US: hypertrophic cardiomyopathy is more common in the US whereas arrhythmogenic right ventricular dysplasia is more common in Italy.
- The annual death rate of 1:27,000 athletes at the initiation of the study is high compared to other studies, an this initial death rate accounts for much of the reduction seen over the course of the study,
- The lowest death rate reported in this study was 0.4 deaths per 100,000 person-years, and is similar to the 0.44 per 100,000 person-years reported for US high school and college students in the US between 1983 and 1993.
- women were underrepresented in this study
But one thing seems clear to me. An ECG is a remarkably simple and non-invasive test to evaluate the heart. Right ventricular abnormalities, chamber enlargement or ventricular hypertrophy, abnormal electrical pathways (Wolff-Parkinson-White syndrome), repolarization abnormalities (congenital Long QT Syndrome) and arrhythmias can be readily detected. Physical examination often cannot detect these subtle killers. And while this study is not conclusive and has significant limitations, it serves as the most potent longitudinal study to date of the value of screening to prevent death in our young athletes.
The addition of the ECG to screening of athletes, given this study’s data, should be seriously considered. For a small cost, It might just save a young athlete’s life and keep me off the front page of the Chicago Tribune.
-Wes
Tuesday, October 03, 2006
Most Athletic Schools
I suppose if "beer curls" were part of the fitness evaluation, the assessment of the 25 most athletic schools would have been harder to differentiate.
--Wes
--Wes
Medical Blogger's Grand Rounds - Vol 3, No. 2
It's up at Rdoctor Medical. Great job, Dr. Kavokin.
And next week's Grand Rounds will be hosted by Unbounded Medicine. For submissions contact j o n m i k e l (AT) g m a i l . c o m.
- Wes
And next week's Grand Rounds will be hosted by Unbounded Medicine. For submissions contact j o n m i k e l (AT) g m a i l . c o m.
- Wes
Monday, October 02, 2006
Of Pigeons and Parades
He stared at the bar and placed his beak upon it. Tap, Tap. Out came a pellet. Tap. A pellet. Tap, tap, tap, another pellet. Tap, tap, tap, tap, tap, tap, a pellet. Tap. A pellet. Tap, tap, tap, tap, tap, tap, tap, tap, tap, tap, finally, a pellet.
Vicarious reinforcement. B.F. Skinner knew in his experiments that a pigeon randomly reinforced, would repeatedly attempt to perform a task multiple times as long as a reward was thought possible. The poor pigeon didn’t want to do anything else.
Isn’t this like education today? Our kids have learned to “press the bar” to assure admission to colleges and medical schools. But on the way, are these kids really the people we want caring for us?
Justin Pope of the Associated Press recently interviewed Marilee Jones, the MIT dean of admissions.
These issues were brought to light for me this past weekend as I attended my 30th high school reunion. One of our activities as the Class of 1976 was to ride a float in the Homecoming parade. The entire town had come out to support the high school there. Sure it was a bit like Mayberry RFD, but it remained a concrete demonstration of the community’s support of their children.
Unfortunately, such an event does not occur here on the North Shore of Chicago at my kids’ high school, New Trier High School, in the posh Winnetka, IL suburb of Chicago. There is no community-sponsored parade, pep rally, or bon fire. Oh, there’s a polite dance for the kids carefully scrutinized by chaperones, but a day-time pep rally or parade involving “down-time” for just fun and community spirit, well that doesn’t exist in our town. It seems the kids are too busy learning or participating in their important college-application-building activities. Such activities used to exist. Why don’t they any longer? Probably because of an accident once during a pep rally eighteen years ago – it might be too dangerous!
Well it might be too dangerous NOT to have them either.
Many of our kids do not get eight hours of sleep a night, or eat three meals a day. Few spend time staring into space and dreaming. As Jones says:
Hopefully, we’ll all see the light. Kids really do need non-judgmental time and space. Community reinforcement and support for all they’re trying to accomplish during these formative years seems like a good idea, too. Just think of the benefits: less pressure might mean less anxiety disorders, fewer teen suicides, cuttings, and sports injuries.
And I really don’t want a determined pigeon-like creature caring for me when I get older.
Tap, tap, tap, tap, tap, tap, tap, tap, tap.
--Wes
Vicarious reinforcement. B.F. Skinner knew in his experiments that a pigeon randomly reinforced, would repeatedly attempt to perform a task multiple times as long as a reward was thought possible. The poor pigeon didn’t want to do anything else.
Isn’t this like education today? Our kids have learned to “press the bar” to assure admission to colleges and medical schools. But on the way, are these kids really the people we want caring for us?
Justin Pope of the Associated Press recently interviewed Marilee Jones, the MIT dean of admissions.
The quest for perfection “is making our children sick,” she told a recent gathering of college admissions professionals in Boston. She means it literally, snapping off statistics on the increase in ulcers, anxiety disorders and control disorders such as cutting and anorexia.And I see it, too. Kids are no longer permitted the luxury of summer camp canoeing or camping – no, it seems they have to now attend scouting camps for sports, summertime science camps, “gifted kid camps” instead on the faint hope that they might make next years’ team. And some will, but many more will not. It’s the “tap, tap, tap” of the bar that keeps our kids trying. Unfortunately, anxieties mount as tensions rise.
Jones grew increasingly worried about the applications that crossed her desk. The students were remarkably accomplished, but she worried the resume rat race had quashed creativity. MIT faculty told her that the students just weren’t much fun to teach. The issue of perfectionism had been brought to the fore at MIT by a series of student suicides.Tap, tap, tap, tap, tap.
These issues were brought to light for me this past weekend as I attended my 30th high school reunion. One of our activities as the Class of 1976 was to ride a float in the Homecoming parade. The entire town had come out to support the high school there. Sure it was a bit like Mayberry RFD, but it remained a concrete demonstration of the community’s support of their children.
Unfortunately, such an event does not occur here on the North Shore of Chicago at my kids’ high school, New Trier High School, in the posh Winnetka, IL suburb of Chicago. There is no community-sponsored parade, pep rally, or bon fire. Oh, there’s a polite dance for the kids carefully scrutinized by chaperones, but a day-time pep rally or parade involving “down-time” for just fun and community spirit, well that doesn’t exist in our town. It seems the kids are too busy learning or participating in their important college-application-building activities. Such activities used to exist. Why don’t they any longer? Probably because of an accident once during a pep rally eighteen years ago – it might be too dangerous!
Well it might be too dangerous NOT to have them either.
Many of our kids do not get eight hours of sleep a night, or eat three meals a day. Few spend time staring into space and dreaming. As Jones says:
”We’re raising a generation of kids trained to please adults. Every day kids should have time when they’re not being judged. That’s the big difference with this generation. They’re being judged and graded and analyzed and assessed at every turn. It’s too much pressure for them.”And time spent stuffing tissue into chicken wire to make a float? Not productive enough – hard to chart a career path out of that one.
Hopefully, we’ll all see the light. Kids really do need non-judgmental time and space. Community reinforcement and support for all they’re trying to accomplish during these formative years seems like a good idea, too. Just think of the benefits: less pressure might mean less anxiety disorders, fewer teen suicides, cuttings, and sports injuries.
And I really don’t want a determined pigeon-like creature caring for me when I get older.
Tap, tap, tap, tap, tap, tap, tap, tap, tap.
--Wes
Subscribe to:
Posts (Atom)